

Fulminant myocarditis associated with the H1N1 influenza virus: case report and literature review
- PMID: 25295829
- PMCID: PMC4188471
- DOI: 10.5935/0103-507x.20140046
Fulminant myocarditis associated with the H1N1 influenza virus: case report and literature review
Abstract
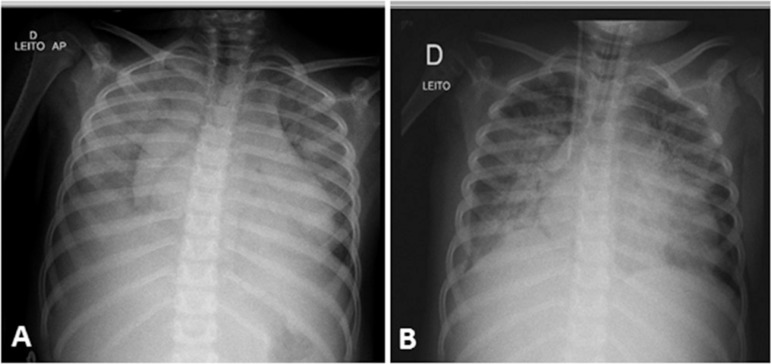
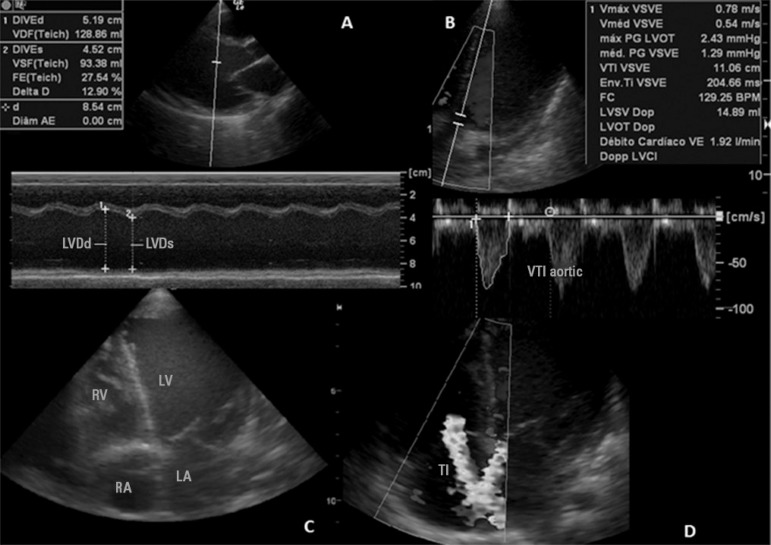
A case of fulminant myocarditis associated with the H1N1 influenza virus. This case report describes the patient's clinical course and emphasizes the importance of bedside echocardiography as an aid in the early diagnosis and management of children with severe myocardial dysfunction. It also discusses aspects relevant to the treatment and prognosis of fulminant myocarditis. The patient was a female, 4 years and 8 months old, previously healthy and with a history of flu symptoms in the past two weeks. The patient was admitted to the emergency room with signs of hemodynamic instability, requiring ventilatory support and vasoactive drugs. The laboratory tests, chest X-ray and echocardiogram suggested the presence of myocarditis. The test for H1N1 in nasopharyngeal secretions was positive. The patient evolved to refractory cardiogenic shock despite the clinical measures applied and died 48 hours after admission to the intensive care unit. The H1N1 influenza virus is an etiological agent associated with acute myocarditis, but there are few reported cases of fulminant myocarditis caused by the H1N1 virus. The identification of signs and symptoms suggestive of fulminant progression should be immediate, and bedside echocardiography is a useful tool for the early detection of myocardial dysfunction and for therapeutic guidance. The use of immunosuppressive therapy and antiviral therapy in acute myocarditis of viral etiology is controversial; hence,the treatment is based on hemodynamic and ventilatory support. The use of hemodynamic support by extracorporeal membrane oxygenation emerges as a promising treatment.
Caso de miocardite fulminante associada ao vírus influenza H1N1, em que foi descrita a evolução clínica do paciente e enfatizada a importância do ecocardiograma à beira do leito como auxílio no diagnóstico precoce e manejo de crianças com disfunção miocárdica grave, além de terem sido discutidos aspectos relevantes relacionados à terapêutica e ao prognóstico da miocardite fulminante. Trata-se de paciente do sexo feminino, 4 anos e 8 meses, previamente hígida, com história de quadro gripal há 2 semanas. Admitida no pronto-socorro com sinais de instabilidade hemodinâmica, necessitando de suporte ventilatório e drogas vasoativas. Exames laboratoriais, radiografia de tórax e ecocardiograma sugestivos de miocardite. Pesquisa positiva para H1N1 em secreção de nasofaringe. Evoluiu com choque cardiogênico refratário a despeito das medidas clínicas, indo a óbito em 48 horas após admissão na unidade de terapia intensiva. O vírus influenza H1N1 é agente etiológico associado a quadros de miocardite aguda, porém poucos são os casos relatados de miocardite fulminante pelo vírus H1N1. A identificação de sinais e sintomas sugestivos de evolução fulminante deve ser imediata e o ecocardiograma à beira do leito é uma ferramenta útil para detecção precoce de disfunção miocárdica e orientação terapêutica. O uso de terapia imunossupressora, em casos de miocardite fulminante de etiologia viral, é controverso, bem como o de terapia antiviral, de tal forma que o tratamento baseia-se em suporte hemodinâmico e ventilatório. O uso de suporte hemodinâmico, por meio de oxigenação por membrana extracorpórea, aparece como terapia promissora.
Conflict of interest statement
Figures
Comment in
-
To: Fulminant myocarditis associated with the H1N1 influenza virus: case report and literature review.Rev Bras Ter Intensiva. 2015 Jan-Mar;27(1):82-3. doi: 10.5935/0103-507X.20150014. Epub 2015 Mar 1. Rev Bras Ter Intensiva. 2015. PMID: 25909318 Free PMC article. No abstract available.
-
Authors' response.Rev Bras Ter Intensiva. 2015 Jan-Mar;27(1):83-4. Rev Bras Ter Intensiva. 2015. PMID: 26103641 English, Portuguese. No abstract available.
References
-
- Saji T, Matsuura H, Hasegawa K, Nishikawa T, Yamamoto E, Ohki H, et al. Comparison of the clinical presentation, treatment, and outcome of fulminant and acute myocarditis in children. Circ J. 2012;76(5):1222–1228. - PubMed
-
- Mamas MA, Fraser D, Neyses L. Cardiovascular manifestations associated with influenza virus infection. Int J Cardiol. 2008;130(3):304–309. - PubMed
-
- Fineberg HV. Pandemic preparedness and response-lessons from the H1N1 influenza of 2009. N Engl J Med. 2014;370(14):1335–1342. - PubMed
-
- Bratincsák A, El-Said HG, Bradley JS, Shayan K, Grossfeld PD, Cannavino CR. Fulminant myocarditis associated with pandemic H1N1 influenza A virus in children. J Am Coll Cardiol. 2010;55(9):928–929. - PubMed
-
- Feldman AM, McNamara D. Myocarditis. N Engl J Med. 2000;343(19):1388–1398. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
