

Imaging adults on extracorporeal membrane oxygenation (ECMO)
- PMID: 25296619
- PMCID: PMC4263804
- DOI: 10.1007/s13244-014-0357-x
Imaging adults on extracorporeal membrane oxygenation (ECMO)
Abstract
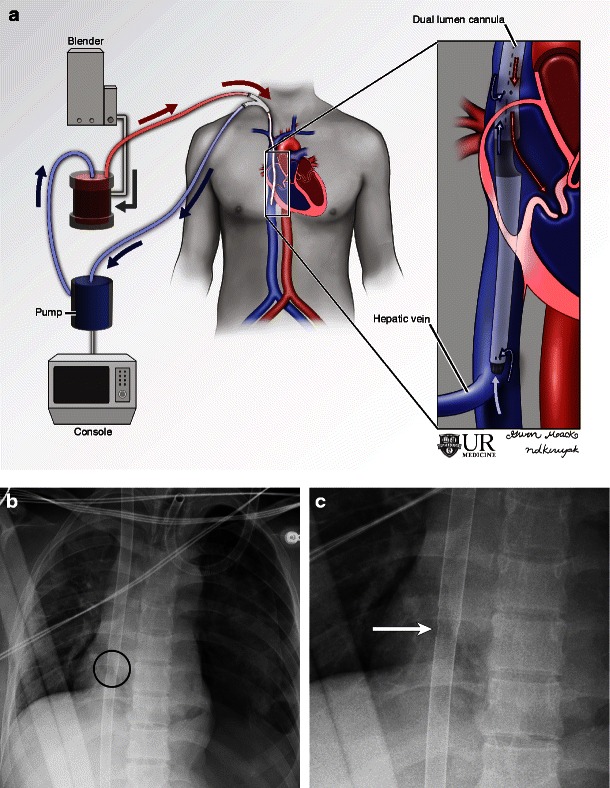
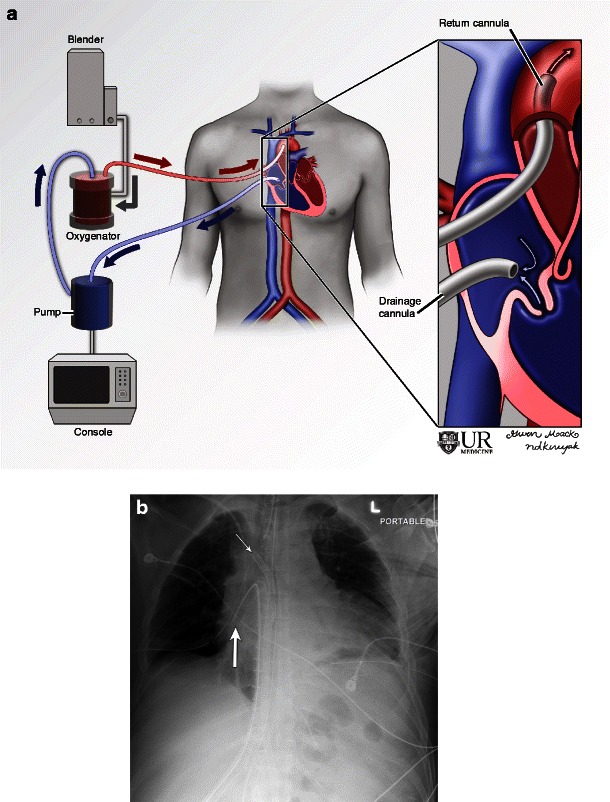
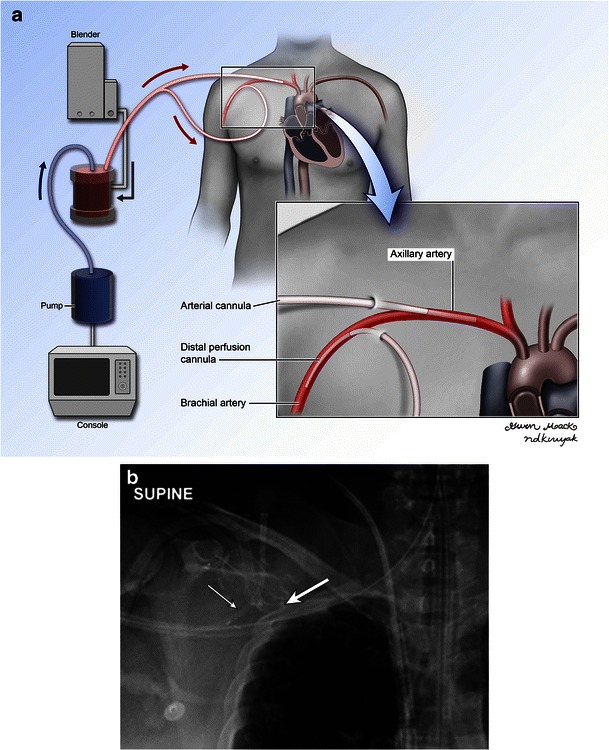
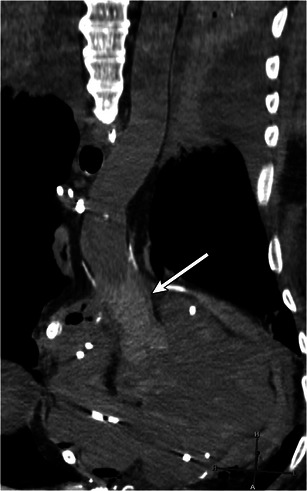
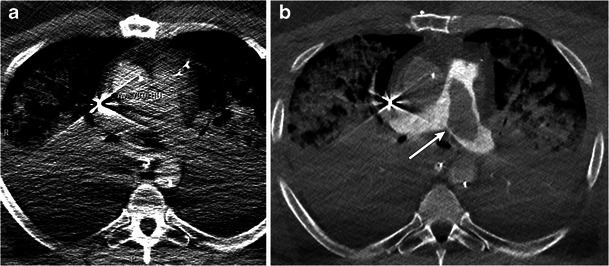
Extracorporeal membrane oxygenation (ECMO) is increasingly being used in adults following failure to wean from cardiopulmonary bypass, after cardiac surgery or in cases of severe respiratory failure. Knowledge of the different types of ECMO circuits, expected locations of cannulas and imaging appearance of complications is essential for accurate imaging interpretation and diagnosis. Commonly encountered complications are malposition of cannulas, adjacent or distal haemorrhage, stroke, stasis thrombus in access vessels, and distal emboli. This article will describe the imaging appearance of different ECMO circuits in adults as well as commonly encountered complications. If a CT (computed tomography) angiogram is being performed on these patients to evaluate for pulmonary embolism, the scan may be suboptimal from siphoning off of the contrast by the ECMO. In such cases, an optimal image can be obtained by lowering the flow rate of the ECMO circuit or by disabling the circuit for the duration of image acquisition. Key Points • Femoroatrial VV ECMO: femoral vein drainage cannula and right atrial return cannula. • Femorofemoral VV ECMO: return and drainage cannulas placed in femoral veins. • Dual-lumen single cannula VV ECMO: via the right IJ/Femoral vein with the tip in the IVC/SVC. • Peripheral VA ECMO: peripheral venous drainage cannula and peripheral arterial return cannula. • Central VA ECMO: direct right atrial drainage cannula and aortic return cannula.
Figures






References
-
- Organization ELS (2014) ELSO website, under registry information. [website] 2014 [cited 2014; Available from: http://www.elso.org/index.php?option=com_content&view=article&id=95&Item....
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
