

Laparoscopic versus open liver resection for hepatocellular carcinoma at a North-American Centre: a 2-to-1 matched pair analysis
- PMID: 25297815
- PMCID: PMC4368393
- DOI: 10.1111/hpb.12342
Laparoscopic versus open liver resection for hepatocellular carcinoma at a North-American Centre: a 2-to-1 matched pair analysis
Abstract
Introduction: Oncological implications of laparoscopic resection in primary hepatic malignancy are not well defined. Laparoscopic liver resection (LLR) for hepatocellular carcinoma (HCC) in comparison to an open liver resection (OLR) in peri-operative and long-term oncological outcomes are described from a single North American institution.
Methods: From 2006 to 2013, all forty-three LLR patients for HCC were evaluated. Each patient was matched to two OLR patients for age at operation, maximal tumour size and tumour number.
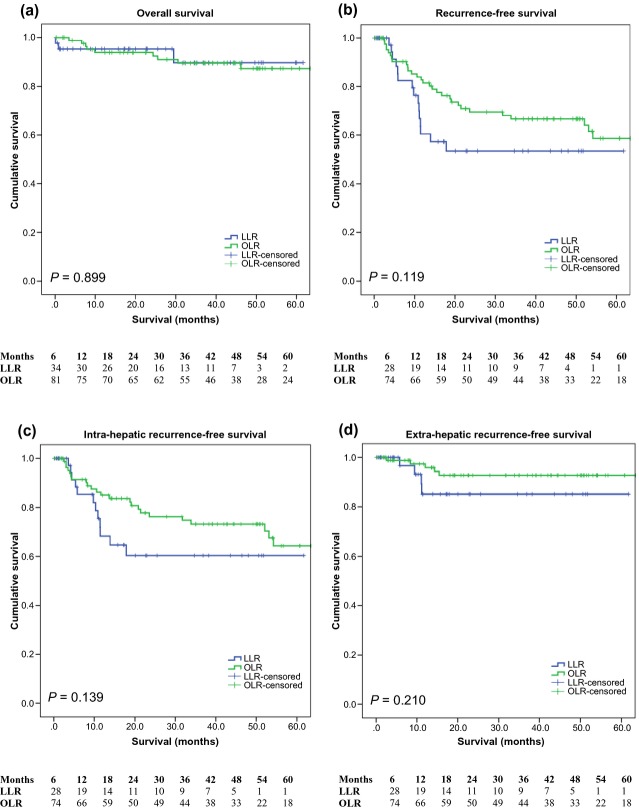
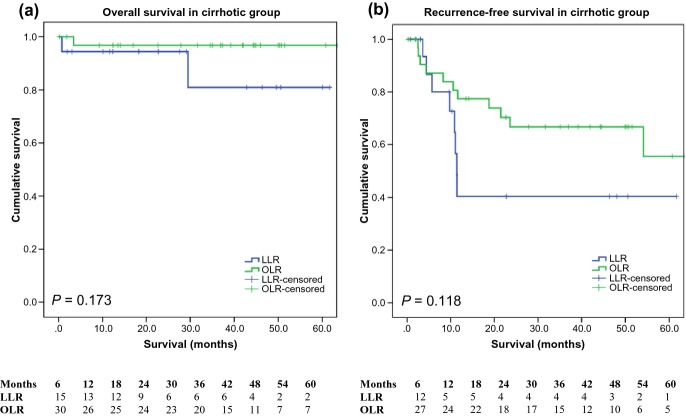
Results: When compared with OLR, LLR had a lower severity of complication (0% versus 27%, P = 0.050) and lower 30-day readmission rate (2.3% versus 18.6%, P = 0.010). The length of stay (LOS) was shorter in LLR patients (5 versus 7 days, P < 0.001) and the estimated blood loss was also lower in LLR (300 versus 700 ml, P = 0.004). Admission to intensive care unit (ICU), emergency room (ER) visits and complication rates were similar. Overall, recurrence-free and intra-hepatic recurrence-free survival were comparable between LLR and OLR.
Discussion: LLR confers the widely-accepted benefits of laparoscopic surgery, namely severity of complication, 30-day readmission rate, LOS and blood loss. Further studies are required to examine intra- and extra-hepatic recurrence after LLR. LLR for HCC should be considered for appropriately selected patients in centres with requisite volume and expertise.
© 2014 International Hepato-Pancreato-Biliary Association.
Figures
References
-
- Bosch FX, Ribes J, Diaz M, Cleries R. Primary liver cancer: worldwide incidence and trends. Gastroenterology. 2004;127:S5–16. - PubMed
-
- Rahbari NN, Mehrabi A, Mollberg NM, Muller SA, Koch M, Buchler MW, et al. Hepatocellular carcinoma: current management and perspective for the future. Ann Surg. 2011;253:453–469. - PubMed
-
- Davila JA, Morgan RO, Shaib Y, McGlyn KA, El-serag HB. Hepatitis C infection and the increasing incidence of hepatocellular carcinoma: a population-based study. Gastroenterology. 2004;127:1372–1380. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
