

The self-adjusting file (SAF) system: An evidence-based update
- PMID: 25298639
- PMCID: PMC4174698
- DOI: 10.4103/0972-0707.139820
The self-adjusting file (SAF) system: An evidence-based update
Abstract
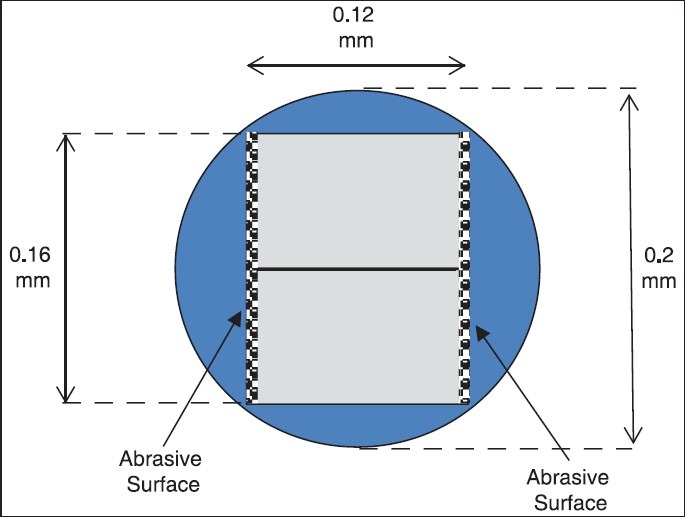
Current rotary file systems are effective tools. Nevertheless, they have two main shortcomings: They are unable to effectively clean and shape oval canals and depend too much on the irrigant to do the cleaning, which is an unrealistic illusionThey may jeopardize the long-term survival of the tooth via unnecessary, excessive removal of sound dentin and creation of micro-cracks in the remaining root dentin. The new Self-adjusting File (SAF) technology uses a hollow, compressible NiTi file, with no central metal core, through which a continuous flow of irrigant is provided throughout the procedure. The SAF technology allows for effective cleaning of all root canals including oval canals, thus allowing for the effective disinfection and obturation of all canal morphologies. This technology uses a new concept of cleaning and shaping in which a uniform layer of dentin is removed from around the entire perimeter of the root canal, thus avoiding unnecessary excessive removal of sound dentin. Furthermore, the mode of action used by this file system does not apply the machining of all root canals to a circular bore, as do all other rotary file systems, and does not cause micro-cracks in the remaining root dentin. The new SAF technology allows for a new concept in cleaning and shaping root canals: Minimally Invasive 3D Endodontics.
Keywords: Cleaning and shaping; NiTi files; SAF; instrumentation; irrigation; minimally invasive; obturation; root filling; rotary files; self-adjusting file.
Conflict of interest statement
Figures





























References
-
- de Chevigny C, Dao TT, Basrani BR, Marquis V, Farzaneh M, Abitbol S, et al. Treatment outcome in endodontics: The Toronto study-phase 4: initial treatment. J Endod. 2008;34:258–63. - PubMed
-
- Molander A, Caplan D, Bergenholtz G, Reit C. Improved quality of root fillings provided by general dental practitioners educated in nickel-titanium rotary instrumentation. Int Endod J. 2007;40:254–60. - PubMed
-
- Larsen CM, Watanabe I, Glickman GN, He J. Cyclic fatigue analysis of a new generation of nickel titanium rotary instruments. J Endod. 2009;35:401–3. - PubMed
-
- Al-Hadlaq SM, Aljarbou FA, AlThumairy RI. Evaluation of cyclic flexural fatigue of Mwire nickel-titanium rotary instruments. J Endod. 2010;36:305–7. - PubMed
-
- Peters OA, Peters CI, Schönenberger K, Barbakow F. ProTaper rotary root canal preparation: Effects of canal anatomy on final shape analysed by micro CT. Int Endod J. 2003;36:86–92. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
