

How can we improve management of syncope in the Emergency Department?
- PMID: 25299508
- PMCID: PMC5110209
- DOI: 10.5603/CJ.a2014.0074
How can we improve management of syncope in the Emergency Department?
Abstract
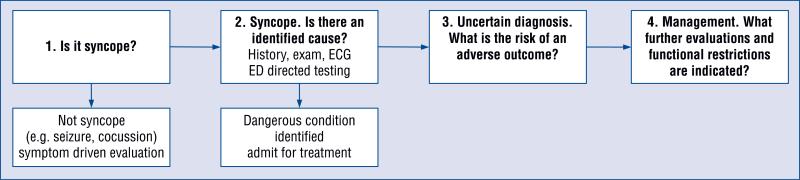
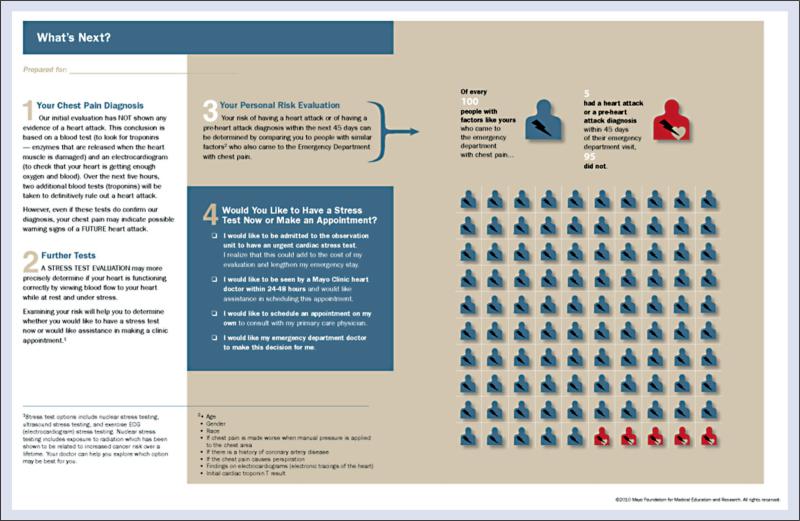
Syncope is a common and challenging presenting complaint to the Emergency Department (ED). Despite substantial research efforts, there is still considerable uncertainty about the optimal ED management of syncope. There is continued interest among clinicians and researchers in improving diagnostic algorithms and optimizing resource utilization. In this paper, we discuss 4 strategies to improve the emergency care of syncope patients: (1) Development of accurate and consistent risk-stratification, (2) Increased use of syncope observation protocols, (3) Evaluation of a discharge with ambulatory monitoring pathway, (4) Use of shared decision-making for disposition decisions. Since current risk-stratification tools have fallen short with regard to subsequent validation and implementation into clinical practice, we outline key factors for future risk-stratification research. We propose that observation units have the potential to safely decrease length-of-stay and hospital costs for hemodynamically stable, intermediate risk patients without adversely affecting clinical outcomes. For appropriate patients with a negative ED evaluation, we recommend consideration of direct discharge, with ambulatory monitoring and expedited follow-up, as a means of decreasing costs and reducing iatrogenic harms. Finally, we advocate for the use of shared decision-making regarding the ultimate disposition of select, intermediate risk patients who have not had a serious condition revealed in the ED. If properly implemented, these four strategies could significantly improve the care of ED syncope patients by helping clinicians identify truly high-risk patients, decreasing unnecessary hospitalizations, and increasing patient satisfaction.
Figures
References
-
- Sun BC, Emond JA, Camargo CA., Jr. Characteristics and admission patterns of patients presenting with syncope to U.S. emergency departments, 1992–2000. Acad Emerg Med. 2004;11:1029–1034. - PubMed
-
- Sun BC, Emond JA, Camargo CA., Jr. Direct medical costs of syncope-related hospitalizations in the United States. Am J Cardiol. 2005;95:668–671. - PubMed
-
- Linzer M, Yang EH, Estes NA, 3rd, Wang P, Vorperian VR, Kapoor WN. Diagnosing syncope. Part 1: Value of history, physical examination, and electrocardiography. Clinical Efficacy Assessment Project of the American College of Physicians. Ann Int Med. 1997;126:989–996. - PubMed
-
- Linzer M, Yang EH, Estes NA, 3rd, Wang P, Vorperian VR, Kapoor WN. Diagnosing syncope. Part 2: Unexplained syncope. Clinical Efficacy Assessment Project of the American College of Physicians. Ann Int Med. 1997;127:76–86. - PubMed
-
- Sarasin FP, Hanusa BH, Perneger T, Louis-Simonet M, Rajeswaran A, Kapoor WN. A risk score to predict arrhythmias in patients with unexplained syncope. Acad Emerg Med. 2003;10:1312–1317. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
