

The 2013 ACC/AHA cardiovascular prevention guidelines improve alignment of statin therapy with coronary atherosclerosis as detected by coronary computed tomography angiography
- PMID: 25299966
- PMCID: PMC5939942
- DOI: 10.1016/j.atherosclerosis.2014.09.023
The 2013 ACC/AHA cardiovascular prevention guidelines improve alignment of statin therapy with coronary atherosclerosis as detected by coronary computed tomography angiography
Abstract
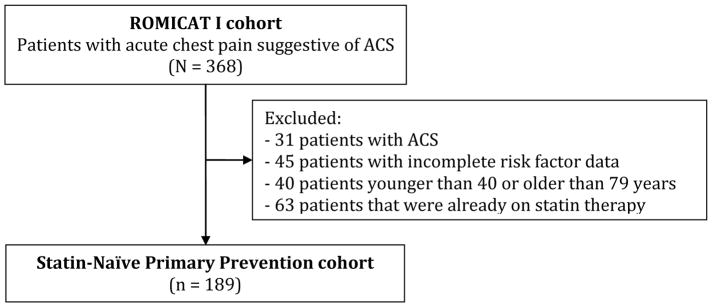
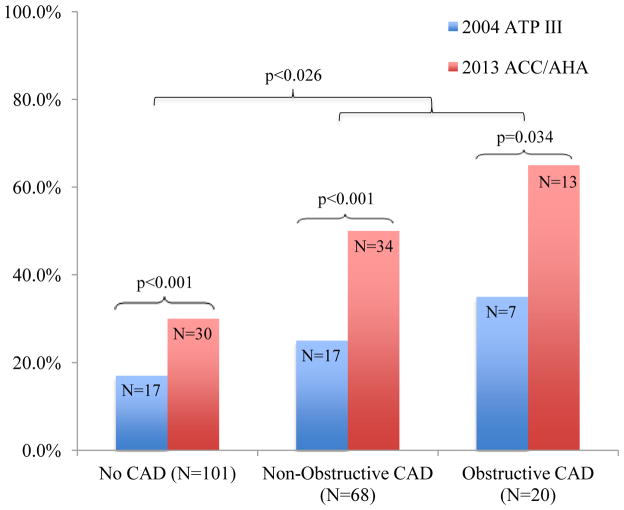
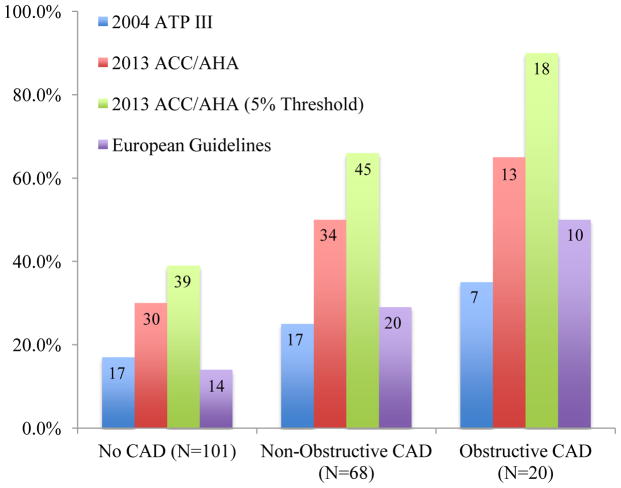
The recently released 2013 ACC/AHA guidelines for management of blood cholesterol have substantially increased the number of adults who are eligible for preventive statin therapy. We sought to determine whether eligibility for statin therapy as determined by the 2013 ACC/AHA guideline recommendation is better aligned with the actual presence of coronary artery disease (CAD) as detected by coronary CT angiography (CCTA) when compared to prior guidelines including the 2004 NCEP ATP III and 2011 ESC/EAS guidelines. In this secondary analysis of the prospective observational ROMICAT I (Rule Out Myocardial Infarction with Computer Assisted Tomography) cohort study, we included all men and women aged 40-79 years presenting with acute chest pain but not diagnosed with acute coronary syndrome nor on admission statin. Based on risk factor assessment and lipid data, we determined guideline-based eligibility for statin therapy by the 2013 ACC/AHA, the 2004 NCEP ATP III, and the 2011 ESC/EAS guidelines. We determined the presence and severity of CAD as detected by CCTA. The 2013 ACC/AHA algorithm identified nearly twice as many individuals as eligible for statins (n = 77/189; 41%) as compared to the 2004 ATP III criteria: (n = 41/189; 22%), (p < .0001) In addition, the 2013 ACC/AHA guidelines were more sensitive for treatment of CCTA-detected CAD than the 2004 ATP III guidelines [53.4% (42.5-64.1) vs 27.3% (18.3-37.8), p < .001] and the 2011 ESC/EAE guidelines [53.4% (42.5-64.1) vs 34.1% (24.3-45.0), p < .001]. However, the specificity of these guidelines was modestly reduced compared to the 2004 ATP III guidelines [70.3 (60.4-79.0) vs 83.2 (74.4-89.9), p < .001] and the 2011 ESC/EAE guidelines [70.3 (60.4-79.0) vs 86.1 (77.8-92.2), p < .001], suggesting increased treatment of subjects without CCTA-detected CAD. Overall, the 2013 ACC/AHA guidelines are more sensitive to identify patients who have CAD detected by CCTA eligible for statin therapy as compared with prior guidelines, with an acceptable trade-off in specificity for recommending statin therapy in those without CAD.
Keywords: Atherosclerosis; Computed tomography; Guidelines; Prevention; Statin.
Copyright © 2014 Elsevier Ireland Ltd. All rights reserved.
Figures
References
-
- Stone NJ, Robinson J, Lichtenstein AH, Bairey Merz CN, Lloyd-Jones DM, Blum CB, McBride P, Eckel RH, Schwartz JS, Goldberg AC, Shero ST, Gordon D, Smith SC, Jr, Levy D, Watson K, Wilson PW. 2013 ACC/AHA Guideline on the Treatment of Blood Cholesterol to Reduce Atherosclerotic Cardiovascular Risk in Adults: A Report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol. 2013 - PubMed
-
- Goff DC, Jr, Lloyd-Jones DM, Bennett G, O’Donnell CJ, Coady S, Robinson J, D’Agostino RB, Sr, Schwartz JS, Gibbons R, Shero ST, Greenland P, Smith SC, Jr, Lackland DT, Sorlie P, Levy D, Stone NJ, Wilson PW. 2013 ACC/AHA Guideline on the Assessment of Cardiovascular Risk: A Report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol. 2013 - PMC - PubMed
-
- Grundy SM, Cleeman JI, Merz CN, Brewer HB, Jr, Clark LT, Hunninghake DB, Pasternak RC, Smith SC, Jr, Stone NJ. Implications of recent clinical trials for the National Cholesterol Education Program Adult Treatment Panel III Guidelines. J Am Coll Cardiol. 2004;44:720–732. - PubMed
-
- Guallar E, Laine C. Controversy Over Clinical Guidelines: Listen to the Evidence, Not the Noise. Ann Intern Med. 2014 - PubMed
-
- Martin SS, Blumenthal RS. Concepts and Controversies: The 2013 American College of Cardiology/American Heart Association Risk Assessment and Cholesterol Treatment Guidelines. Ann Intern Med. 2014 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
