

The retrieval of unerupted teeth in pedodontics: two case reports
- PMID: 25301242
- PMCID: PMC4206860
- DOI: 10.1186/1752-1947-8-334
The retrieval of unerupted teeth in pedodontics: two case reports
Abstract
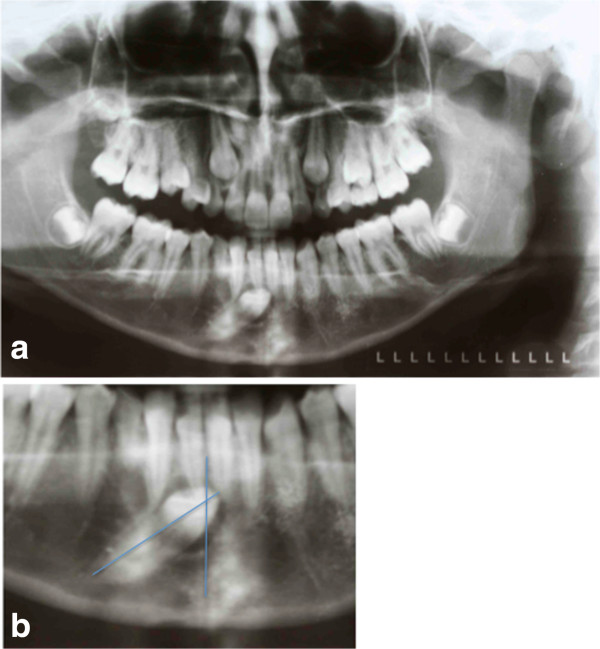
Introduction: The retrieval of unerupted teeth in pedodontics is always significant to preserve the trophism of adjacent tissues, establish the correct space, provide adequate function and maintain good esthetics for the patient. The treatment plan is based on radiographic examinations and measurements, and on an accurate clinical evaluation; it aims to achieve the best treatment possible depending on the complexity of the specific case.In the most difficult clinical cases it is very important to have an early diagnosis, which is essential to plan the treatment and achieve success. In these cases, the pediatrician is in a strategic position to give an early diagnosis through a child's medical history and by counting the child's teeth.
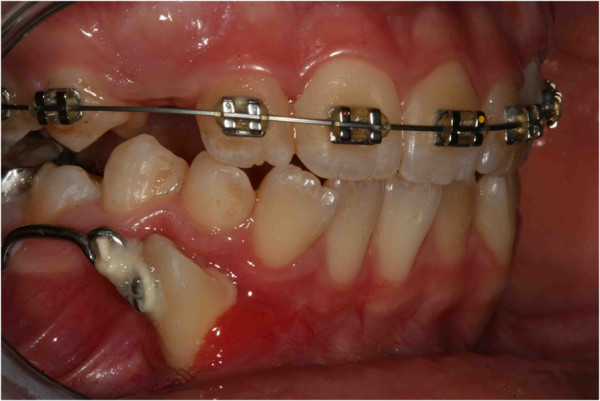
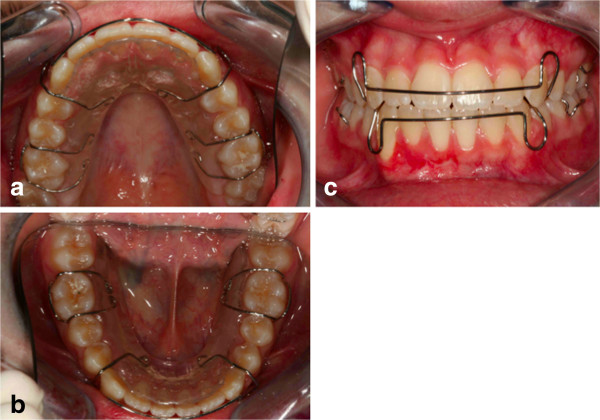
Case presentation: This article presents two different difficult clinical cases of impacted teeth diagnosed during pediatric age, with a radiological analysis, and successfully treated with orthodontic devices designed for these specific cases. Clinical case 1 describes a 13-year-old Italian girl; clinical case 2 describes a 9-year-old Italian girl. The use of these devices achieved the desired treatment goals. The problems associated with impacted teeth and the biomechanical interventions used for these patients are discussed.
Conclusions: An early and careful diagnosis followed by an accurate treatment plan for the individual cases can lead to retrieval of the impacted teeth without affecting other anatomic structures and adjacent teeth. In these cases, the pediatrician is in a strategic position to give an early diagnosis through a child's medical history and by counting the child's teeth.
Figures


























References
-
- Almonaitiene R, Balciuniene I, Tutkuviene J. Factors influencing permanent teeth eruption. Part one – general factors. Stomatologija. 2010;12(3):67–72. Review. - PubMed
-
- Albani F, Ballesio I, Campanella V, Marzo G. Pit and fissure sealants: results at five and ten years. Eur J Paediatr Dent. 2005;6(2):61–65. - PubMed
-
- Valletta G, Matarasso S, Mignogna M. Malattie Odontostomatologiche. Piccin: Milano; 2005.
-
- Andreasen JO. In: Textbook and Color Atlas of Tooth Impactions. Andreasen JO, Kolsen Petersen J, Laskin DM, editor. Copenhagen: Munksgaard; 1997. Treatment strategies for eruption disturbances. Chapter 3; pp. 65–91.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
