

Sex differences in cardiovascular outcome during progression of aortic valve stenosis
- PMID: 25301859
- PMCID: PMC4316939
- DOI: 10.1136/heartjnl-2014-306078
Sex differences in cardiovascular outcome during progression of aortic valve stenosis
Abstract
Objective: Women with severe aortic valve stenosis (AS) have better LV systolic function and more concentric LV geometry than their male counterparts. However, sex differences in cardiovascular (CV) outcome during progression of AS have not been reported from a longitudinal prospective study.
Methods: Doppler echocardiography and CV events were recorded during a median of 4.0 years in 979 men and 632 women aged 28-86 (mean 67±10) years in the Simvastatin Ezetimibe in Aortic Stenosis (SEAS) study. LV systolic function was assessed by EF and midwall shortening (MWS). Study outcomes were AS-related events, ischaemic CV events and total mortality.
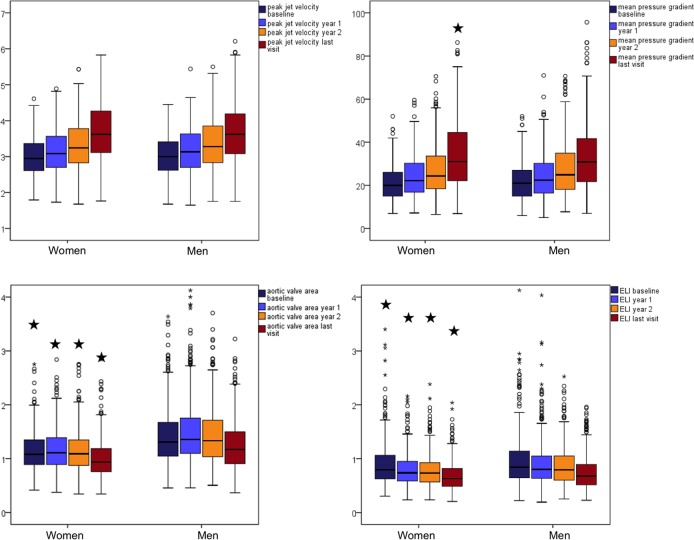
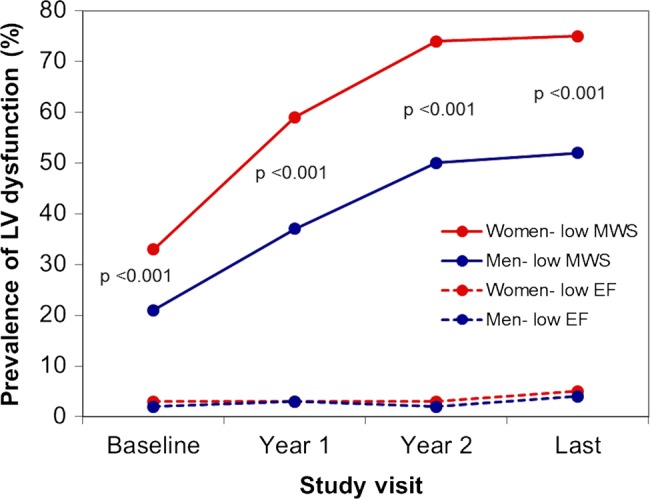
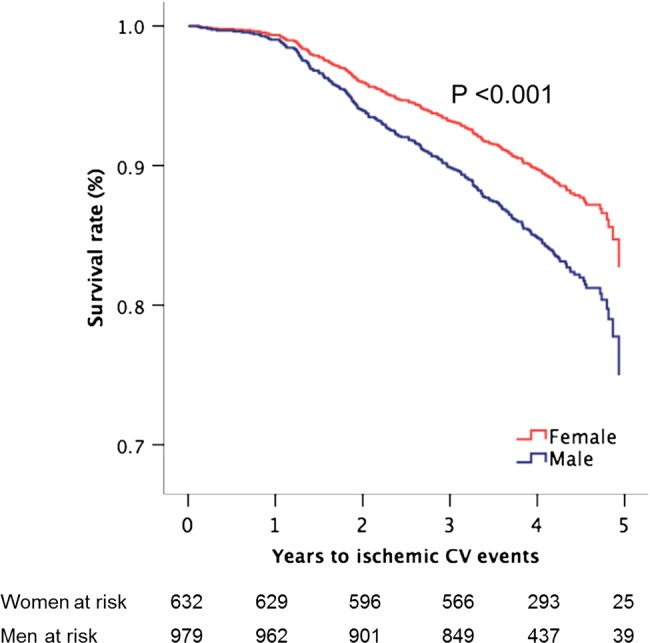
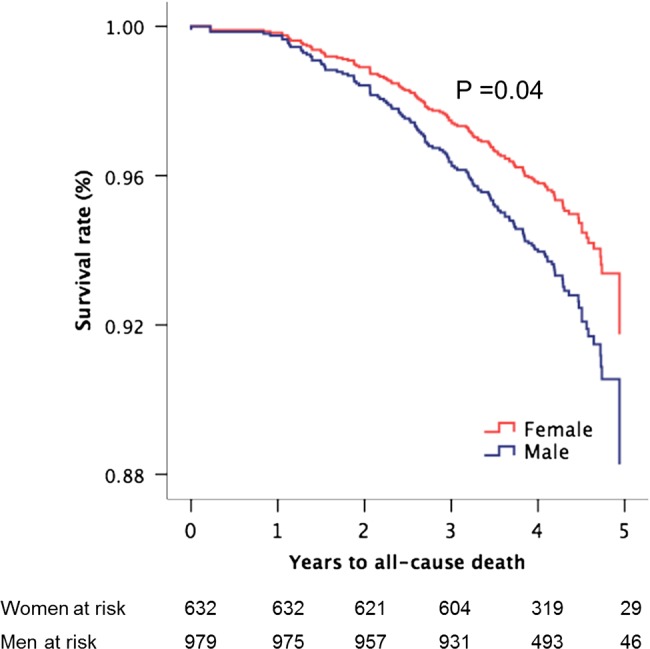
Results: The annular cumulative incidence of AS events, ischaemic CV events and death was 8.1%, 3.4% and 2.8% in women, and 8.9%, 4.4% and 2.4% in men, respectively. Women and men had similar AS progression rate whether measured by peak jet velocity, mean gradient or valve area. In multivariate analyses, female sex independently predicted less reduction in LV MWS and EF during follow-up (both p<0.05). In time-varying Cox analyses, women had a 40% lower rate of ischaemic CV events (95% CI 21% to 54%), in particular, more than 50% lower rate of stroke and coronary artery bypass grafting, and a 31% lower all-cause mortality (95% CI 1% to 51%), independent of active study treatment, age and hypertension, as well as time-varying valve area, low systolic function and abnormal LV geometry. AS event rate did not differ by sex.
Conclusions: In the SEAS study, women and men had similar rates of AS progression and AS-related events. However, women had lower total mortality and ischaemic CV event rate than men independent of confounders.
Trial registration number: ClinicalTrials.gov identifier: NCT00092677.
Published by the BMJ Publishing Group Limited. For permission to use (where not already granted under a licence) please go to http://group.bmj.com/group/rights-licensing/permissions.
Figures
References
-
- Iung B, Baron G, Butchart EG, et al. . A prospective survey of patients with valvular heart disease in Europe: The Euro Heart Survey on Valvular Heart Disease. Eur Heart J 2003;24:1231–43. - PubMed
-
- Nkomo VT, Gardin JM, Skelton TN, et al. . Burden of valvular heart diseases: a population-based study. Lancet 2006;368:1005–11. - PubMed
-
- Otto CM. Valvular aortic stenosis: disease severity and timing of intervention. J Am Coll Cardiol 2006;47:2141–51. - PubMed
-
- Baumgartner H, Hung J, Bermejo J, et al. . Echocardiographic assessment of valve stenosis: EAE/ASE recommendations for clinical practice. J Am Soc Echocardiogr 2009;22:1–23. - PubMed
-
- Aurigemma GP, Silver KH, McLaughlin M, et al. . Impact of chamber geometry and gender on left ventricular systolic function in patients >60 years of age with aortic stenosis. Am J Cardiol 1994;74:794–8. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials