

Immunolocalization of platelet-derived growth factor receptor-β (PDGFR-β) and pericytes in cerebral autosomal dominant arteriopathy with subcortical infarcts and leukoencephalopathy (CADASIL)
- PMID: 25303037
- PMCID: PMC5098250
- DOI: 10.1111/nan.12188
Immunolocalization of platelet-derived growth factor receptor-β (PDGFR-β) and pericytes in cerebral autosomal dominant arteriopathy with subcortical infarcts and leukoencephalopathy (CADASIL)
Abstract
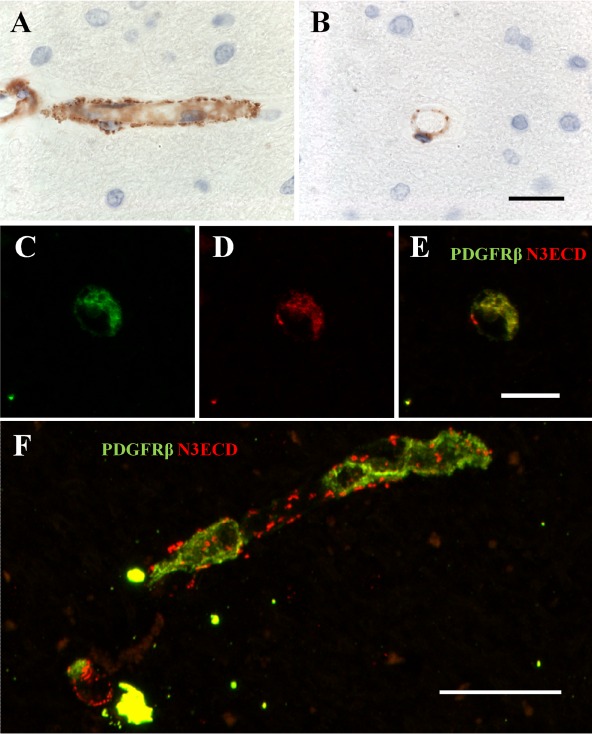
Aims: Cerebral autosomal dominant arteriopathy with subcortical infarcts and leukoencephalopathy (CADASIL) is identified by aggregates of NOTCH3 extracellular domain (N3ECD) along capillaries and the deposition of granular osmiophilic material (GOM). We assessed the pattern of distribution of pericytes in relation to N3ECD deposits in cerebral microvessels of CADASIL subjects.
Methods: We assessed post mortem brains from (n = 50) subjects with CADASIL, cerebral small vessel disease, and similar-age cognitively normal and older controls. Immunohistochemical and immunofluorescent staining methods were used to study the distribution and quantify immunoreactivities of the platelet-derived growth factor receptor-β (PDGFR-β) (for pericytes) and microvascular markers in the frontal cortex and white matter.
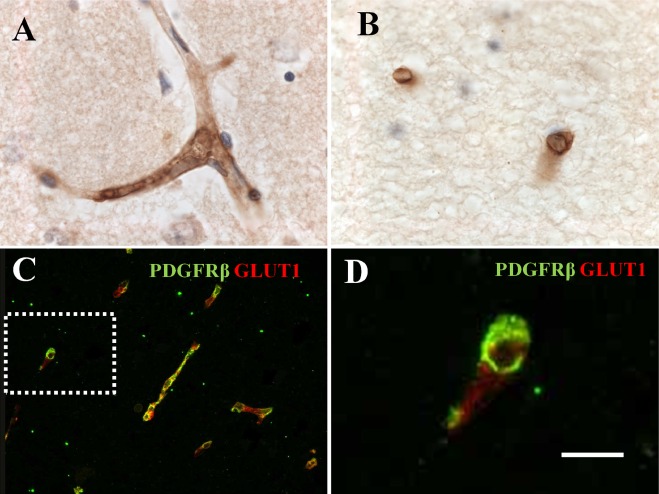
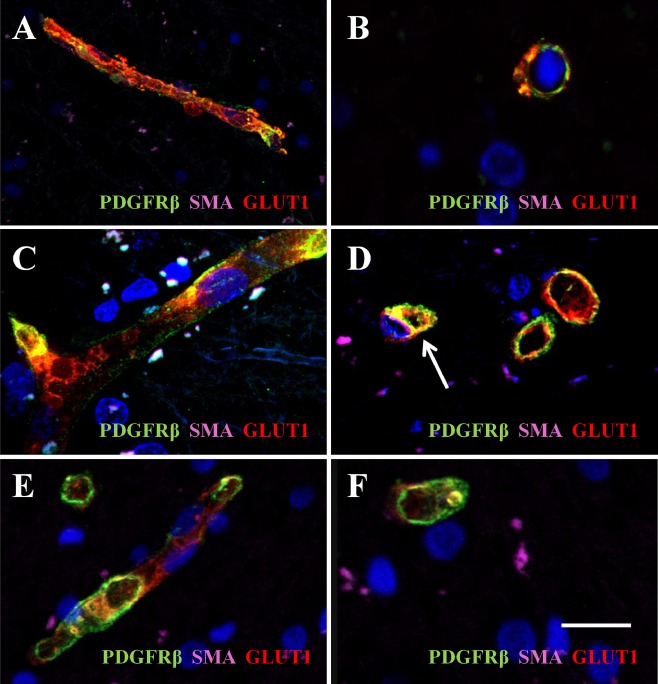
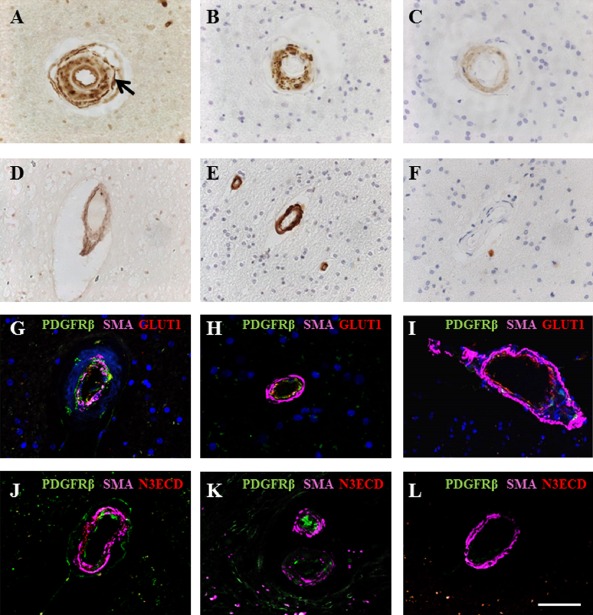
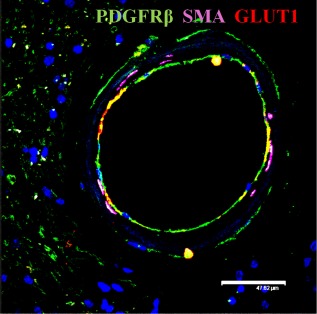
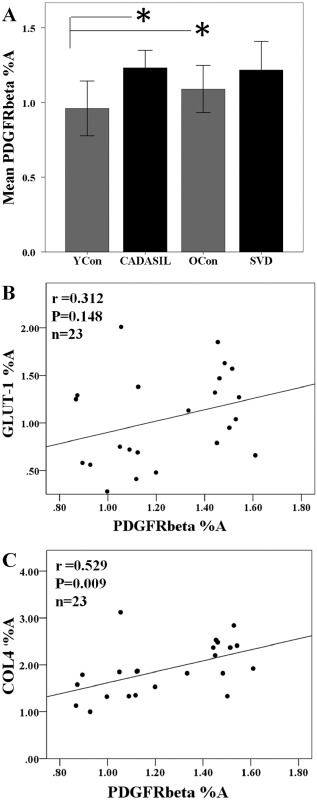
Results: PDGFR-β antibody stained cells typical of pericytes in capillaries and small arterioles in both the grey and white matter. PDGFR-β reactive pericytes adopted 'crescent' morphology wrapped closely around capillary walls readily evident in cross-sections. We noted considerable overlap between PDGFR-β and N3ECD imunoreactivities in capillaries. Quantitative analysis of PDGFR-β immunoreactivity revealed significant differences in PDGFR-β %A in CADASIL compared with young controls (P < 0.05). PDGFR-β %A was further positively correlated with the basement membrane marker collagen IV (r = 0.529, P = 0.009), but was not associated with GLUT-1, the marker for endothelial cells.
Conclusions: Our results suggest increased expression of PDGFR-β immunoreactive pericytes in cerebral microvessels in CADASIL compared with similar age controls. While we cannot confirm whether PDGFR-β-expressing pericytes produce N3ECD and hence GOM, our findings demonstrate that up-regulation of pericyte-like cells is associated with microvascular changes, including loss of vascular smooth muscle cells in CADASIL.
Keywords: CADASIL; capillaries; dementia; pericyte; platelet-derived growth factor receptor; vascular dementia; vascular smooth muscle cell.
© 2014 The Authors. Neuropathology and Applied Neurobiology published by John Wiley & Sons Ltd. on behalf of British Neuropathological Society.
Figures
References
-
- Kalaria RN, Viitanen M, Kalimo H, Dichgans M, Tabira T, Vas‐Cog CGo . The pathogenesis of CADASIL: an update. J Neurol Sci 2004; 226: 35–39 - PubMed
-
- Yamamoto Y, Craggs L, Baumann M, Kalimo H, Kalaria RN. Review: molecular genetics and pathology of hereditary small vessel diseases of the brain. Neuropathol Appl Neurobiol 2011; 37: 94–113 - PubMed
-
- Chabriat H, Joutel A, Dichgans M, Tournier‐Lasserve E, Bousser MG. CADASIL. Lancet Neurol 2009; 8: 643–653 - PubMed
-
- Yamamoto Y, Craggs LJ, Watanabe A, Booth T, Attems J, Low RW, Oakley AE, Kalaria RN. Brain microvascular accumulation and distribution of the NOTCH3 ectodomain and granular osmiophilic material in CADASIL. J Neuropathol Exp Neurol 2013; 72: 416–431 - PubMed
-
- Dziewulska D, Lewandowska E. Pericytes as a new target for pathological processes in CADASIL. Neuropathology 2012; 32: 515–521 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
