

Differences in cardiovascular disease risk when antihypertensive medication adherence is assessed by pharmacy fill versus self-report: the Cohort Study of Medication Adherence among Older Adults (CoSMO)
- PMID: 25304468
- PMCID: PMC4514519
- DOI: 10.1097/HJH.0000000000000382
Differences in cardiovascular disease risk when antihypertensive medication adherence is assessed by pharmacy fill versus self-report: the Cohort Study of Medication Adherence among Older Adults (CoSMO)
Abstract
Background: Pharmacy refill adherence assesses the medication-filling behaviors, whereas self-report adherence assesses the medication-taking behaviors. We contrasted the association of pharmacy refill and self-reported antihypertensive medication adherence with blood pressure (BP) control and cardiovascular disease (CVD) incidence.
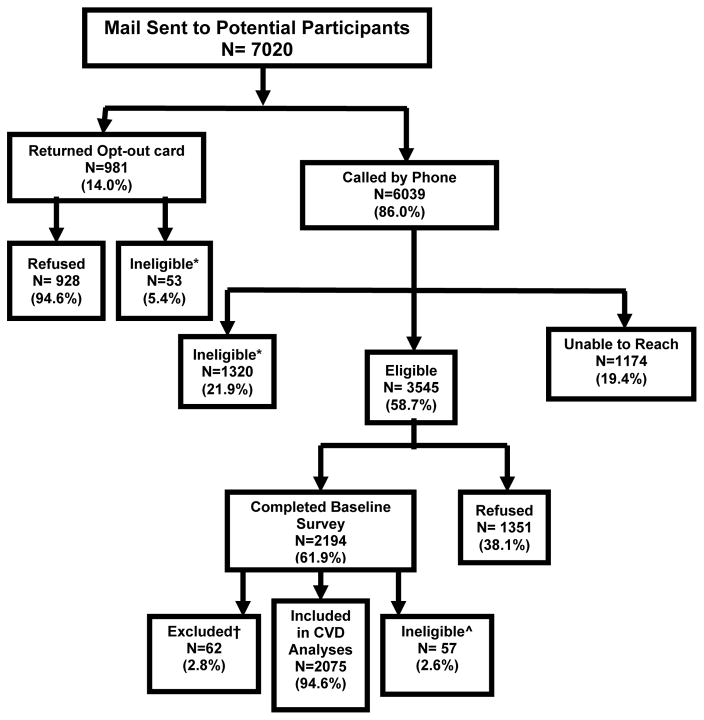
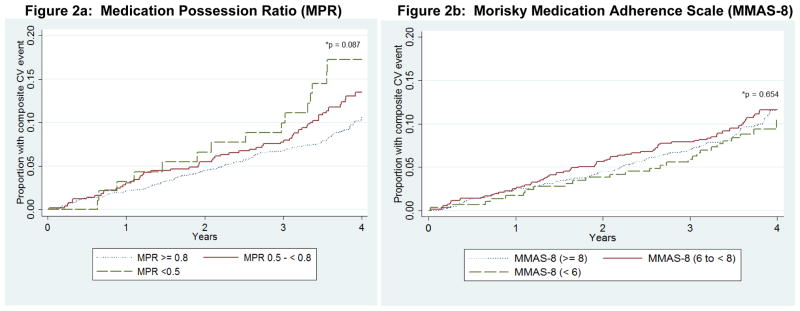
Methods and results: Adults (n = 2075) from the prospective Cohort Study of Medication Adherence among Older Adults recruited between August 2006 and September 2007 were included. Antihypertensive medication adherence was determined using a pharmacy refill measure, medication possession ratio (MPR; low, medium, and high MPR: <0.5, 0.5 to <0.8, and ≥0.8, respectively) and a self-reported measure, eight-item Morisky Medication Adherence Scale (MMAS-8; low, medium, and high MMAS-8: <6, 6 to <8, and 8, respectively). Incident CVD events (stroke, myocardial infarction, congestive heart failure, or CVD death) through February 2011 were identified and adjudicated. The prevalence of low, medium, and high adherence was 4.5, 23.7, and 71.8% for MPR and 14.0, 34.3, and 51.8% for MMAS-8, respectively. During a median of 3.8 years' follow-up, 240 (11.5%) people had a CVD event. Low MPR and low MMAS-8 were associated with uncontrolled BP at baseline and during follow up. After multivariable adjustment and compared to those with high MPR, the hazard ratios for CVD associated with medium and low MPR were 1.17 [95% confidence interval (CI) 0.87-1.56)] and 1.87 (95% CI: 1.06-3.30), respectively. Compared to those with high MMAS-8, the hazard ratios (95% CI) for MMAS-8 for medium and low MMAS-8 were 1.04 (0.79-1.38) and 0.89 (0.58-1.35), respectively.
Conclusion: While both adherence measures were associated with BP control, pharmacy refill but not self-report antihypertensive medication adherence was associated with incident CVD. The differences in these associations may be because of the distinctions in what each adherence measure assesses.
Figures
References
-
- Ezzati M, Lopez AD, Rodgers A, Vander HS, Murray CJ. Selected major risk factors and global and regional burden of disease. Lancet. 2002 Nov 2;360(9343):1347–60. - PubMed
-
- Haynes RB, McDonald HP, Garg AX. Helping patients follow prescribed treatment: clinical applications. JAMA. 2002 Dec 11;288(22):2880–3. - PubMed
-
- Corrao G, Parodi A, Nicotra F, Zambon A, Merlino L, Cesana G, Mancia G. Better compliance to antihypertensive medications reduces cardiovascular risk. J Hypertens. 2011 Mar;29(3):610–8. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
