

Clinical and survival analysis of 36 cases of primary fallopian tube carcinoma
- PMID: 25307473
- PMCID: PMC4200227
- DOI: 10.1186/1477-7819-12-311
Clinical and survival analysis of 36 cases of primary fallopian tube carcinoma
Abstract
Background: Primary fallopian tube carcinoma (PFTC) is rarely seen clinically. Herein, we investigate the clinical and pathological characteristics and appropriate therapies for PFTC.
Methods: A total of 36 patients for whom PFTC was pathologically confirmed from January 2001 to July 2011 in Beijing Hospital of Gynecology and Obstetrics, an affiliate of Capital Medical University, were retrospectively analyzed.
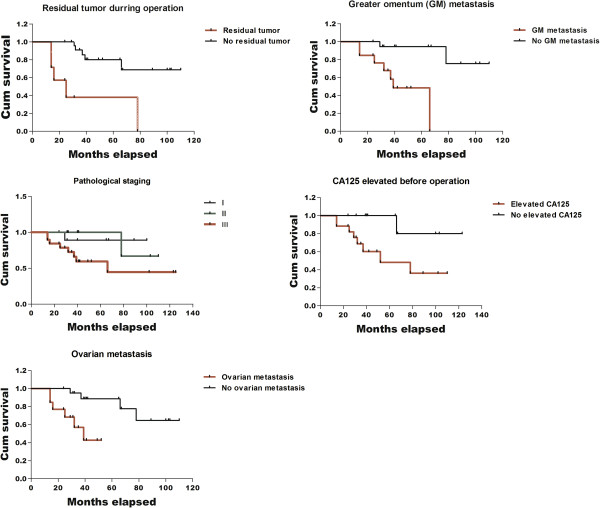
Results: A total of 36 cases underwent surgical staging in our hospital: 47.2% were early stage cases , and 52.8% were advanced stage cases. Of the 36 cases, 24 cases were pure adenocarcinoma, 10 cases were mixed, and there was 1 case of undifferentiated carcinoma, 1 case of undifferentiated carcinoma combined with transitional cell carcinoma, 5 cases of moderately differentiated carcinoma, and 29 cases of moderately to poorly differentiated carcinoma. There were no cases of highly differentiated carcinoma. Among the cases examined, 38.9% (14/36) had omentum metastasis, and 19 cases had an elevated CA125 during a preoperative biochemical laboratory test. Approximately 35 cases received postoperative adjuvant chemotherapy. The 3-year and 5-year overall survival rates for the 36 cases were 80.7% and 65.4%, respectively. Single-factor analysis showed that the pathological conditions of residual tumor diameter >1 cm (P < 0.001), omentum metastasis (P = 0.003), ovary metastasis (P = 0.004) and elevated preoperative CA125 (P = 0.044) were associated with prognosis, whereas pathological surgical staging (P = 0.069), retroperitoneal lymph node metastasis (P = 0.499), and pathological classification (P = 0.183) were not associated with prognosis. Multifactor analysis showed that a residual tumor diameter >1 cm (P = 0.019) and omentum metastasis (P = 0.015) were associated with prognosis, and were, therefore, the independent risk factors of prognosis.
Conclusions: PFTC is a rare female genital tract malignancy. Most patients are in an advanced stage at diagnosis, which results in a poor prognosis. Complete surgical staging and maximal resection should be recommended.
Figures
References
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
