

Establishment of a new prostate cancer multidisciplinary clinic: Format and initial experience
- PMID: 25307625
- PMCID: PMC4270998
- DOI: 10.1002/pros.22904
Establishment of a new prostate cancer multidisciplinary clinic: Format and initial experience
Abstract
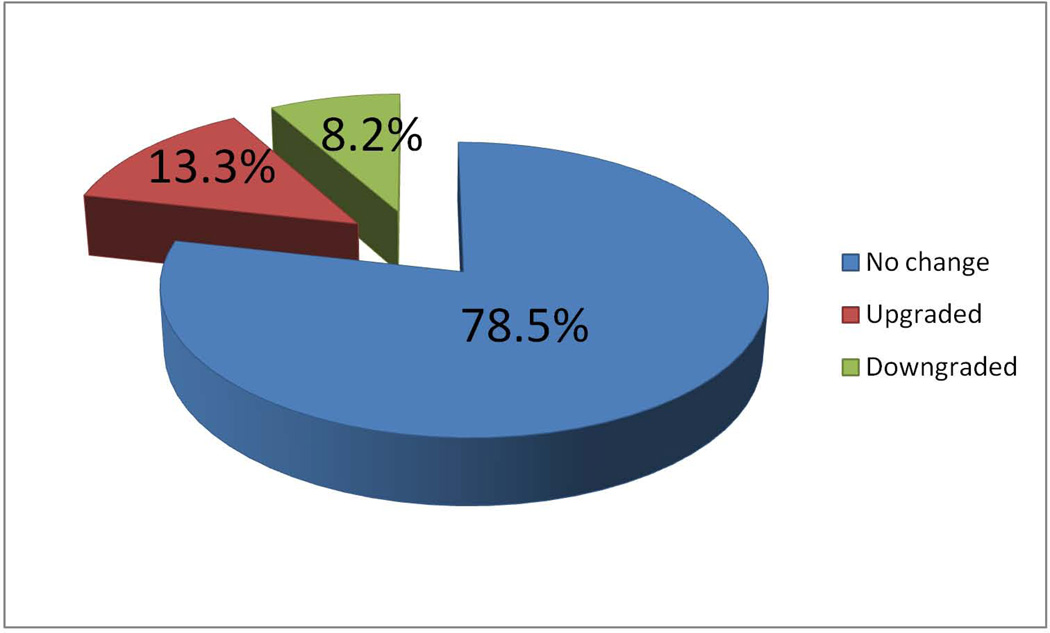
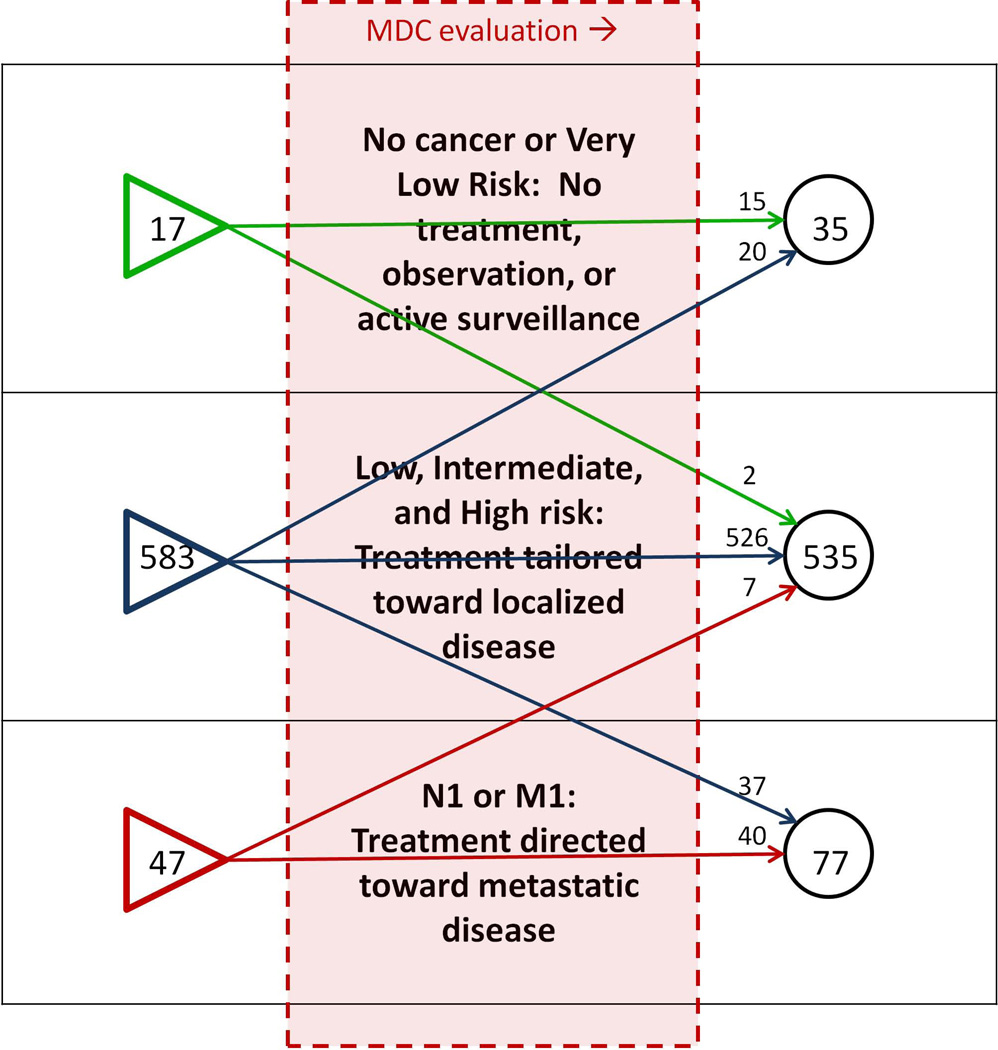
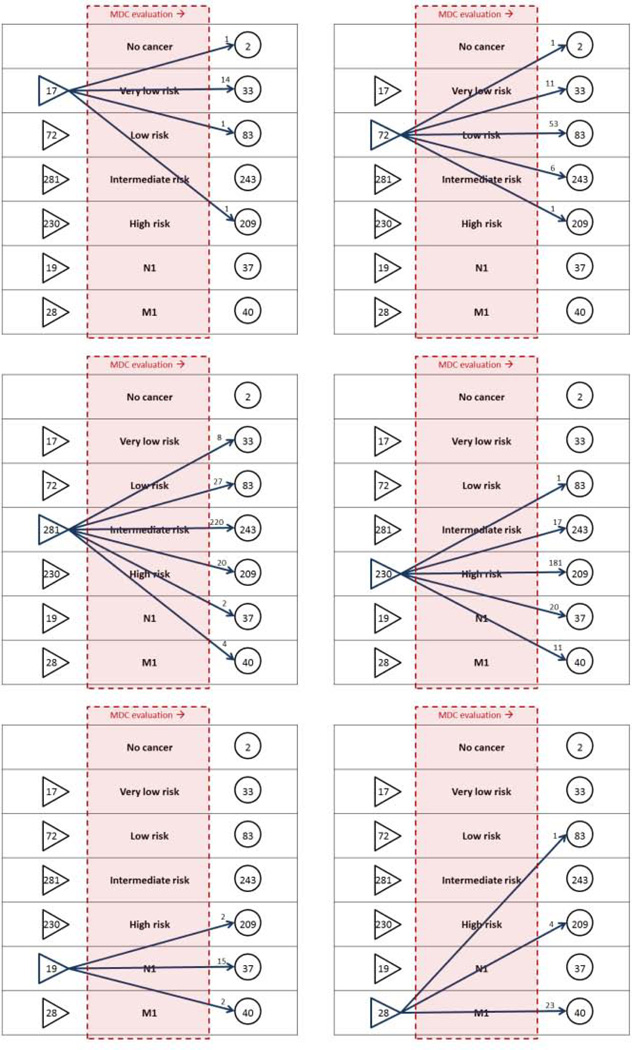
Background: The use of multidisciplinary clinics (MDCs) for outpatient cancer evaluation is increasing. MDCs may vary in format, and data on whether MDCs change prostate cancer (PCa) care are limited. Here we report on the setup and design of a relatively new PCa MDC clinic. Because MDC evaluation was associated with a comprehensive re-evaluation of all patients' staging and risk stratification data, we studied the frequency of changes in PCa grade and stage upon MDC evaluation, which provides a unique estimate of the magnitude of pathology, radiology, and exam-based risk stratification in a modern tertiary setting.
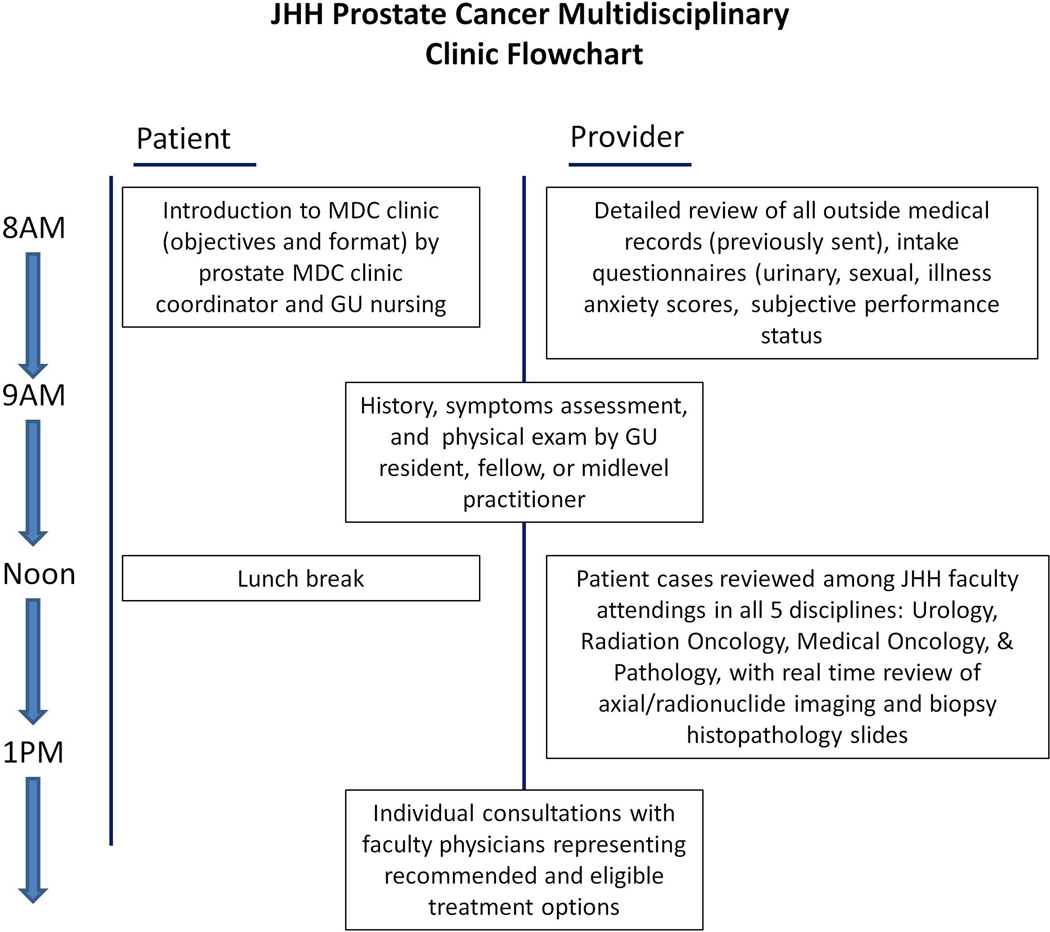
Methods: In 2008-2012, 887 patients underwent consultation for newly diagnosed PCa at the Johns Hopkins Hospital (JHH) weekly MDC. In a same-day process, patients are interviewed and examined in a morning clinic. Examination findings, radiology studies, and biopsy slides are then reviewed during a noon conference that involves real-time collaboration among JHH attending specialty physicians: urologists, radiation oncologists, medical oncologists, pathologists, and radiologists. During afternoon consultations, attending physicians appropriate to each patient's eligible treatment options individually meet with patients to discuss management strategies and/or clinical trials. Retrospective chart review identified presenting tumor characteristics based on outside assessment, which was compared with stage and grade as determined at MDC evaluation.
Results: Overall, 186/647 (28.7%) had a change in their risk category or stage. For example, 2.9% of men were down-classified as very-low-risk, rendering them eligible for active surveillance. 5.7% of men thought to have localized cancer were up-classified as metastatic, thus prompting systemic management approaches. Using NCCN guidelines as a benchmark, many men were found to have undergone non-indicated imaging (bone scan 23.9%, CT/MRI 47.4%). The three most chosen treatments after MDC evaluation were external beam radiotherapy ± androgen deprivation (39.3%), radical prostatectomy (32.0%), and active surveillance/expectant management (12.9%).
Conclusions: A once-weekly same-day evaluation that involves simultaneous data evaluation, management discussion, and patient consultations from a multidisciplinary team of PCa specialists is feasible. Comprehensive evaluation at a tertiary referral center, as demonstrated in a modern MDC setting, is associated with critical changes in presenting disease classification in over one in four men.
Keywords: diagnosis; grading; pathology; radiology; staging.
© 2014 Wiley Periodicals, Inc.
Figures
References
-
- Swain S, Hudis C. Health policy: Upholding the Affordable Care Act--implications for oncology. Nat. Rev. Clin. Oncol. 2012;9(9):491–492. - PubMed
-
- Stewart SB, Bañez LL, Robertson CN, et al. Utilization trends at a multidisciplinary prostate cancer clinic: initial 5-year experience from the Duke Prostate Center. J. Urol. 2012;187(1):103–108. - PubMed
-
- Aizer Aa, Paly JJ, Zietman AL, et al. Multidisciplinary Care and Pursuit of Active Surveillance in Low-Risk Prostate Cancer. J. Clin. Oncol. 2012;30(25) - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
