

Germline variants in the SEMA4A gene predispose to familial colorectal cancer type X
- PMID: 25307848
- PMCID: PMC4214414
- DOI: 10.1038/ncomms6191
Germline variants in the SEMA4A gene predispose to familial colorectal cancer type X
Abstract
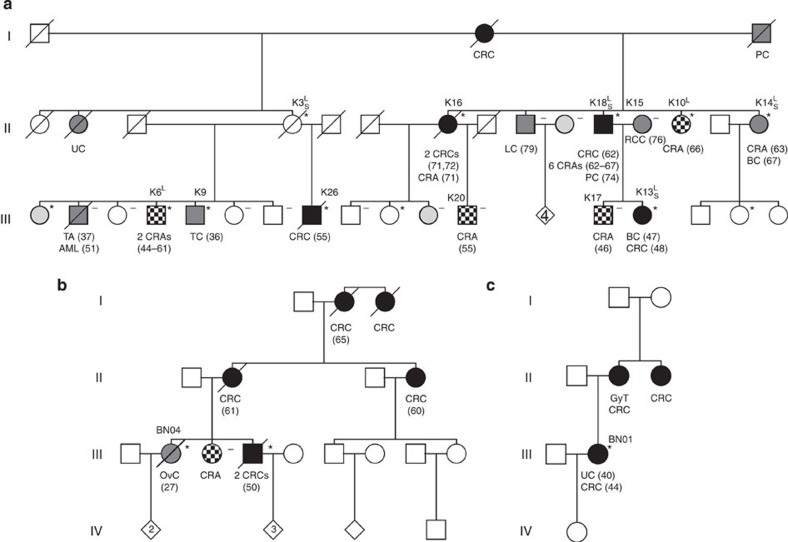
Familial colorectal cancer type X (FCCTX) is characterized by clinical features of hereditary non-polyposis colorectal cancer with a yet undefined genetic background. Here we identify the SEMA4A p.Val78Met germline mutation in an Austrian kindred with FCCTX, using an integrative genomics strategy. Compared with wild-type protein, SEMA4A(V78M) demonstrates significantly increased MAPK/Erk and PI3K/Akt signalling as well as cell cycle progression of SEMA4A-deficient HCT-116 colorectal cancer cells. In a cohort of 53 patients with FCCTX, we depict two further SEMA4A mutations, p.Gly484Ala and p.Ser326Phe and the single-nucleotide polymorphism (SNP) p.Pro682Ser. This SNP is highly associated with the FCCTX phenotype exhibiting increased risk for colorectal cancer (OR 6.79, 95% CI 2.63 to 17.52). Our study shows previously unidentified germline variants in SEMA4A predisposing to FCCTX, which has implications for surveillance strategies of patients and their families.
Figures



Comment in
-
Correspondence: Reply to 'SEMA4A variation and risk of colorectal cancer'.Nat Commun. 2016 Mar 10;7:10695. doi: 10.1038/ncomms10695. Nat Commun. 2016. PMID: 26960273 Free PMC article. No abstract available.
-
Correspondence: SEMA4A variation and risk of colorectal cancer.Nat Commun. 2016 Mar 10;7:10611. doi: 10.1038/ncomms10611. Nat Commun. 2016. PMID: 26961734 Free PMC article. No abstract available.
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
