

Reduced CMRO₂ and cerebrovascular reserve in patients with severe intracranial arterial stenosis: a combined multiparametric qBOLD oxygenation and BOLD fMRI study
- PMID: 25307948
- PMCID: PMC6869377
- DOI: 10.1002/hbm.22657
Reduced CMRO₂ and cerebrovascular reserve in patients with severe intracranial arterial stenosis: a combined multiparametric qBOLD oxygenation and BOLD fMRI study
Abstract
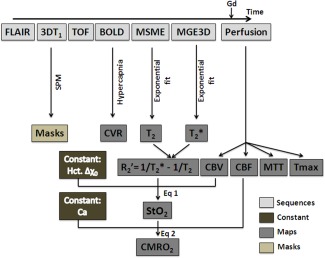
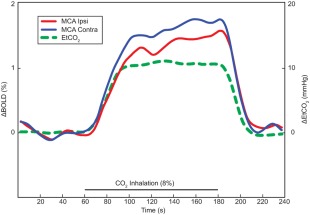
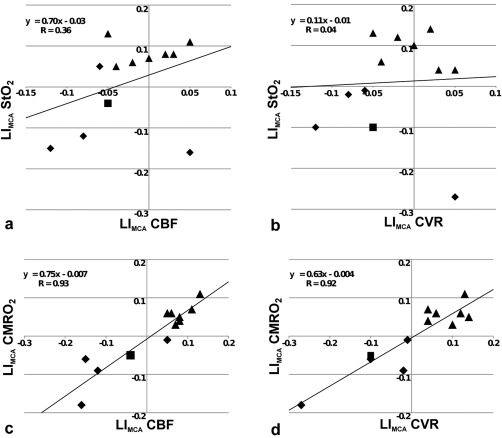
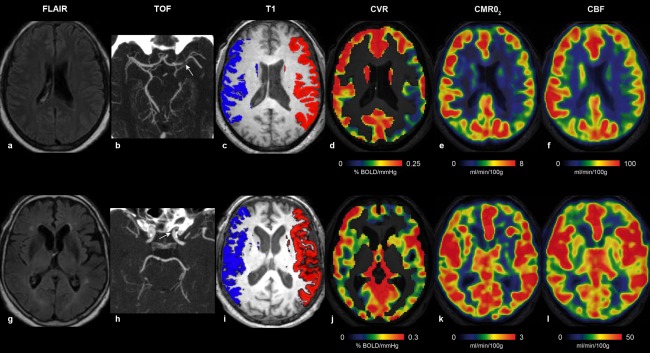
Multiparametric quantitative blood oxygenation level dependent (mqBOLD) magnetic resonance Imaging (MRI) approach allows mapping tissular oxygen saturation (StO2 ) and cerebral metabolic rate of oxygen (CMRO2 ). To identify hemodynamic alteration related to severe intracranial arterial stenosis (SIAS), functional MRI of cerebrovascular reserve (CVR BOLD fMRI) to hypercapnia has been proposed. Diffusion imaging suggests chronic low grade ischemia in patients with impaired CVR. The aim of the present study was to evaluate how oxygen parameters (StO2 and CMRO2 ), assessed with mqBOLD approach, correlate with CVR in patients (n = 12) with SIAS and without arterial occlusion. The perfusion (dynamic susceptibility contrast), oxygenation, and CVR were compared. The MRI protocol conducted at 3T lasted approximately 1 h. Regions of interest measures on maps were delineated on segmented gray matter (GM) of middle cerebral artery territories. We have shown that decreased CVR is spatially associated with decreased CMRO2 in GM of patients with SIAS. Further, the degree of ipsilateral CVR reduction was well-correlated with the amplitude of the CMRO2 deficit. The altered CMRO2 suggests the presence of a moderate ischemia explained by both a decrease in perfusion and in CVR. CVR and mqBOLD method may be helpful in the selection of patients with SIAS to advocate for medical therapy or percutaneous transluminal angioplasty-stenting.
Keywords: BOLD fMRI; brain; cerebral metabolic rate of oxygen (CMRO2); cerebrovascular reserve; hypercapnia; intracranial arterial stenosis; microvasculature; perfusion; stroke; tissular oxygen saturation (StO2).
© 2014 Wiley Periodicals, Inc.
Figures

References
-
- Baron JC, Jones T (2012): Oxygen metabolism, oxygen extraction and positron emission tomography: Historical perspective and impact on basic and clinical neuroscience. NeuroImage 61:492–504. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
