

Hospital and emergency department factors associated with variations in missed diagnosis and costs for patients age 65 years and older with acute myocardial infarction who present to emergency departments
- PMID: 25308132
- PMCID: PMC4285372
- DOI: 10.1111/acem.12486
Hospital and emergency department factors associated with variations in missed diagnosis and costs for patients age 65 years and older with acute myocardial infarction who present to emergency departments
Abstract
Objectives: The objective was to measure the variation in missed diagnosis and costs of care for older acute myocardial infarction (AMI) patients presenting to emergency departments (EDs) and to identify the hospital and ED characteristics associated with this variation.
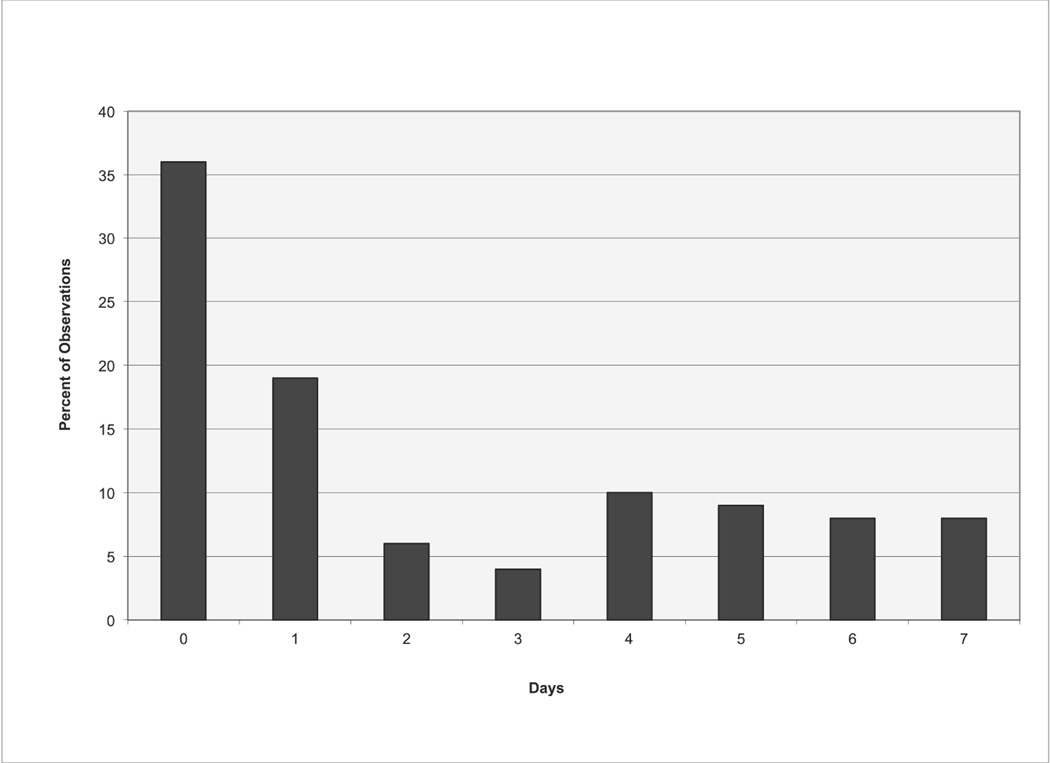
Methods: Using 2004-2005 Medicare inpatient and outpatient records, the authors identified a cohort of AMI patients age 65 years and older who presented to the ED for initial care. The primary outcome was missed diagnosis of AMI, i.e., AMI hospital admission within 7 days of an ED discharge for a condition suggestive of cardiac ischemia. Costs were defined as Medicare hospital payments for all services associated with and immediately resulting from the ED evaluation. The effect of ED and hospital characteristics on quality and costs were estimated using multilevel models with hospital random effects.
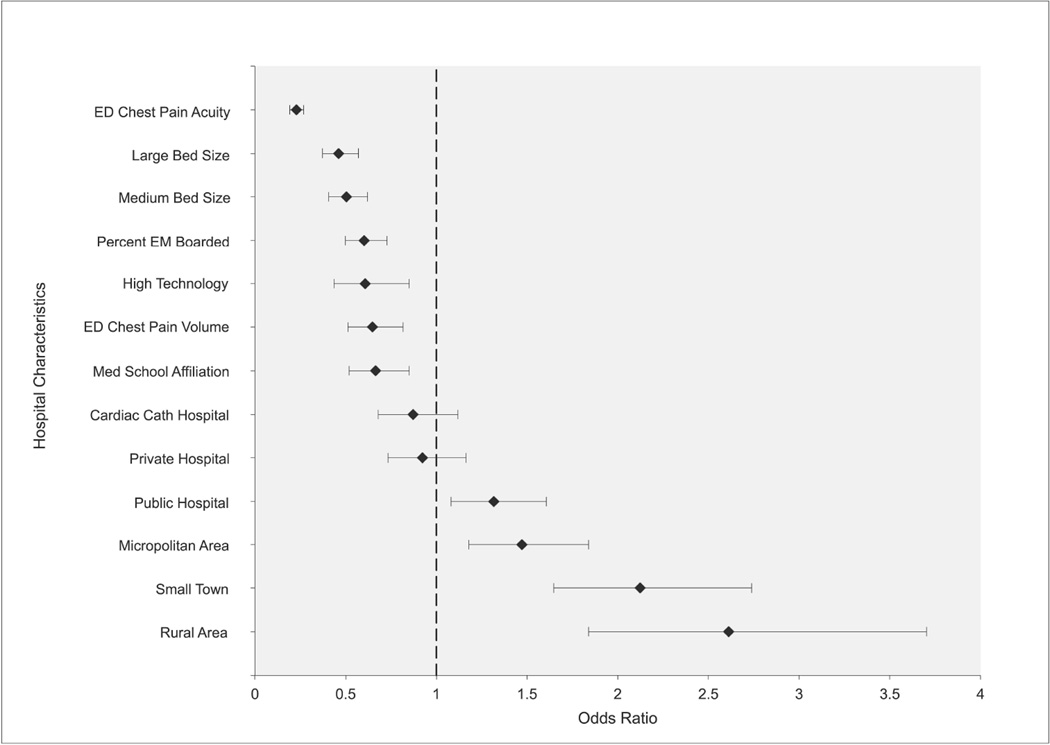
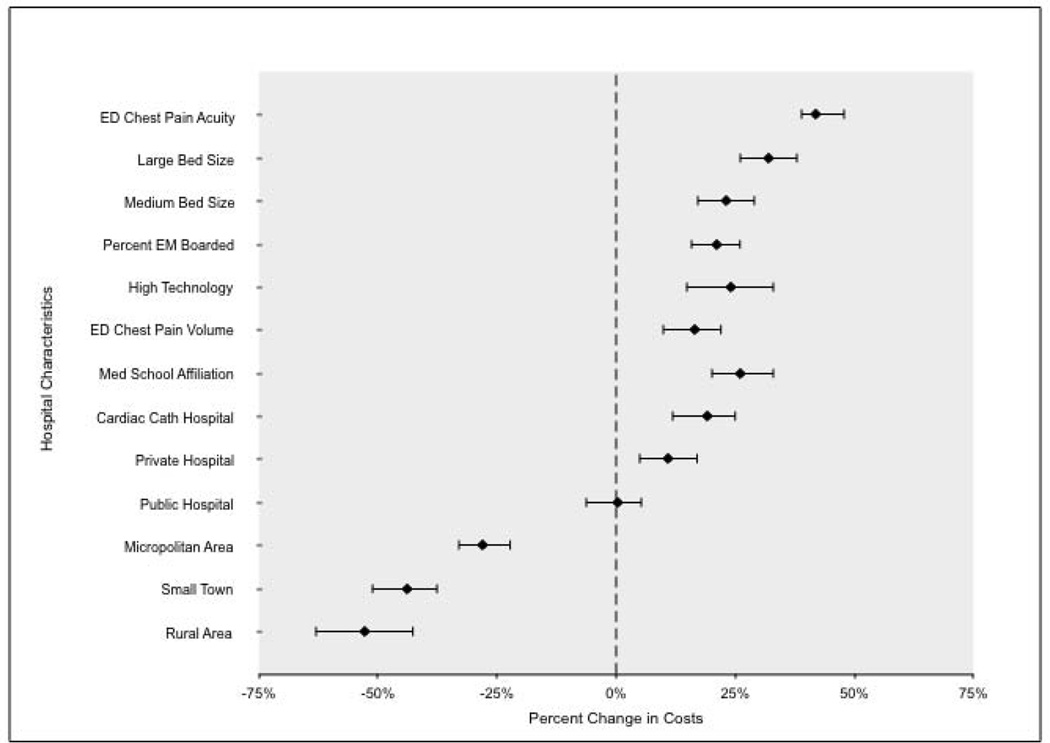
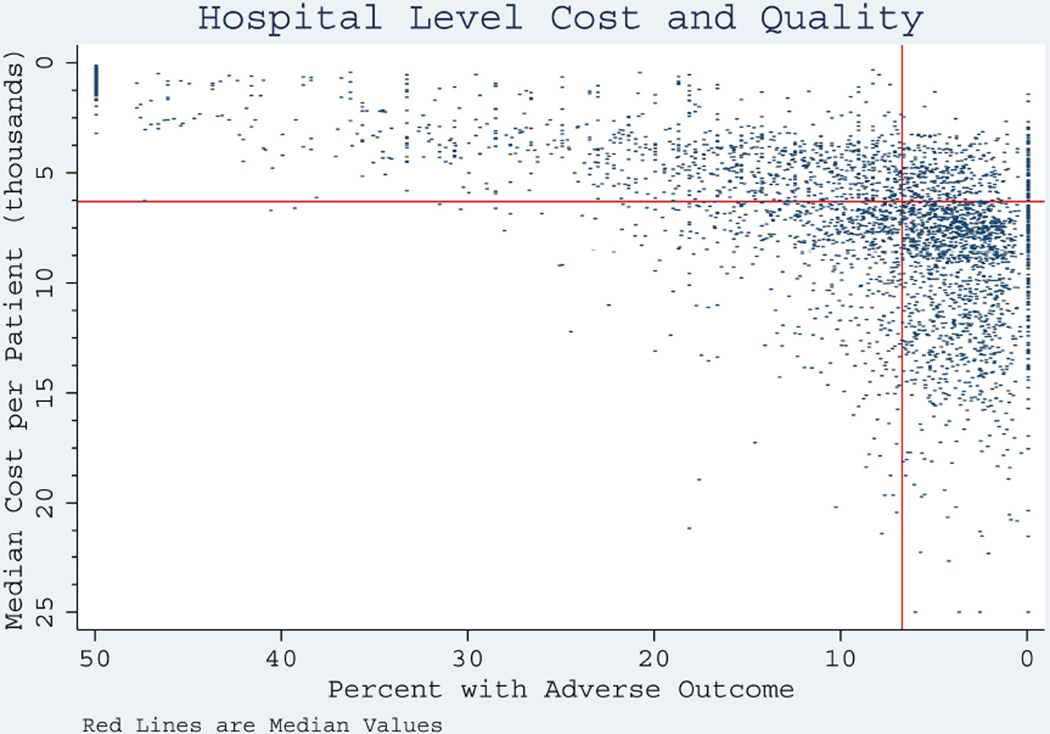
Results: There were 371,638 AMI patients age 65 and older included in the study, of whom 4,707 were discharged home from their initial ED visits and subsequently admitted to the hospital. The median unadjusted hospital-level missed diagnosis percentage was 0.52% (interquartile range [IQR] = 0 to 3.45%). ED characteristics protective of adverse outcomes include higher ED chest pain acuity (adjusted odds ratio [aOR] = 0.23, 99% confidence interval [CI] = 0.19 to 0.27) and American Board of Emergency Medicine (ABEM) certification (aOR = 0.60, 99% CI = 0.50 to 0.73). Protective hospital characteristics include larger hospital size (aOR = 0.46, 99% CI = 0.37 to 0.57) and academic status (aOR = 0.74, 99% CI = 0.58 to 0.94). All of these characteristics were associated with higher costs as well.
Conclusions: The proportion of missed AMI diagnoses and cost of care for patients age 65 years and older presenting to EDs with AMI varies across hospitals. Hospitals with more board-certified emergency physicians (EPs) and higher average acuity are associated with significantly higher quality. All hospital characteristics associated with better ED outcomes are associated with higher costs.
© 2014 by the Society for Academic Emergency Medicine.
Conflict of interest statement
Similar articles
-
Variation in chest pain emergency department admission rates and acute myocardial infarction and death within 30 days in the Medicare population.Acad Emerg Med. 2015 Aug;22(8):955-64. doi: 10.1111/acem.12728. Epub 2015 Jul 23. Acad Emerg Med. 2015. PMID: 26205260
-
The risk of missed diagnosis of acute myocardial infarction associated with emergency department volume.Ann Emerg Med. 2006 Dec;48(6):647-55. doi: 10.1016/j.annemergmed.2006.03.025. Epub 2006 Jun 14. Ann Emerg Med. 2006. PMID: 17112926
-
Unrecognized Cardiovascular Emergencies Among Medicare Patients.JAMA Intern Med. 2018 Apr 1;178(4):477-484. doi: 10.1001/jamainternmed.2017.8628. JAMA Intern Med. 2018. PMID: 29482196 Free PMC article.
-
Chest pain centers: diagnosis of acute coronary syndromes.Ann Emerg Med. 2000 May;35(5):449-61. Ann Emerg Med. 2000. PMID: 10783407 Review.
-
Emergency department factors associated with survival after sudden cardiac arrest.Resuscitation. 2013 Mar;84(3):292-7. doi: 10.1016/j.resuscitation.2012.10.013. Epub 2012 Oct 24. Resuscitation. 2013. PMID: 23103887 Review.
Cited by
-
Racial Disparities in Hospitalization Among Patients Who Receive a Diagnosis of Acute Coronary Syndrome in the Emergency Department.J Am Heart Assoc. 2022 Oct 4;11(19):e025733. doi: 10.1161/JAHA.122.025733. Epub 2022 Sep 21. J Am Heart Assoc. 2022. PMID: 36129027 Free PMC article.
-
Comparing Charlson and Elixhauser comorbidity indices with different weightings to predict in-hospital mortality: an analysis of national inpatient data.BMC Health Serv Res. 2021 Jan 6;21(1):13. doi: 10.1186/s12913-020-05999-5. BMC Health Serv Res. 2021. PMID: 33407455 Free PMC article.
-
Incidence, Relevant Patient Factors, and Clinical Outcomes of the Misdiagnosis of ST-Segment-Elevation Myocardial Infarction: Results From the Korea Acute Myocardial Infarction Registry.J Am Heart Assoc. 2023 Jul 4;12(13):e029728. doi: 10.1161/JAHA.123.029728. Epub 2023 Jun 22. J Am Heart Assoc. 2023. PMID: 37345749 Free PMC article.
-
Diagnostic discrepancies between emergency department admissions and hospital discharges among older adults: secondary analysis on a population-based survey.Sao Paulo Med J. 2020 Sep-Oct;138(5):359-367. doi: 10.1590/1516-3180.0471.R1.05032020. Sao Paulo Med J. 2020. PMID: 32935740 Free PMC article.
-
Emergency medicine in the Veterans Health Administration-results from a nationwide survey.Am J Emerg Med. 2015 Jul;33(7):899-903. doi: 10.1016/j.ajem.2015.03.062. Epub 2015 Apr 6. Am J Emerg Med. 2015. PMID: 25936477 Free PMC article.
References
-
- Mensah GA, Brown DW. An overview of cardiovascular disease burden in the United States. Health Aff (Millwood) 2007;26:38–48. - PubMed
-
- McClellan M. Reforming payments to healthcare providers: the key to slowing healthcare cost growth while improving quality? J Economic Perspectives. 2011;25:69–92. - PubMed
-
- Schuur JD, Venkatesh AK. The growing role of emergency departments in hospital admissions. N Engl J Med. 2012;367:391–393. - PubMed
-
- Lee TH, Rouan GW, Weisberg MC, et al. Clinical characteristics and natural history of patients with acute myocardial infarction sent home from the emergency room. Am J Cardiol. 1987;60:219–224. - PubMed
-
- Pope JH, Aufderheide TP, Ruthazer R, et al. Missed diagnoses of acute cardiac ischemia in the emergency department. N Engl J Med. 2000;342:1163–1170. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
