

Chronic pain treatment in children and adolescents: less is good, more is sometimes better
- PMID: 25308551
- PMCID: PMC4287516
- DOI: 10.1186/1471-2431-14-262
Chronic pain treatment in children and adolescents: less is good, more is sometimes better
Abstract
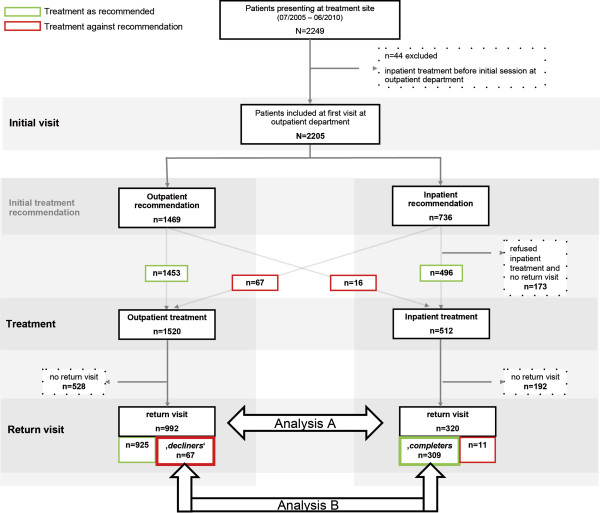
Background: In children with chronic pain, interdisciplinary outpatient and intensive inpatient treatment has been shown to improve pain intensity and disability. However, there are few systematic comparisons of outcomes of the two treatments. The present naturalistic study aimed to compare the clinical presentation and achieved changes at return in three outcome domains (pain intensity, disability, school absence) between a) outpatients vs. inpatients and b) patients who declined intensive inpatient treatment and completed outpatient treatment instead (decliners) vs. those who completed inpatient treatment (completers).
Methods: The study compared treatment outcomes between n = 992 outpatients vs. n = 320 inpatients (Analysis A) who were treated at a tertiary treatment centre and returned for a return visit within a one-year interval. In Analysis B, treatment outcomes were compared between n = 67 decliners vs. n = 309 completers of inpatient treatment. The three outcome domains were compared by calculating standardized change scores and clinically significant changes.
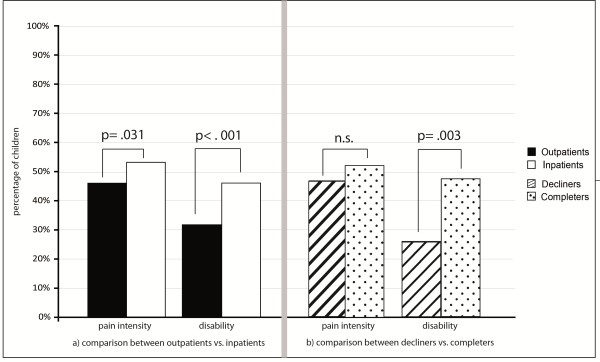
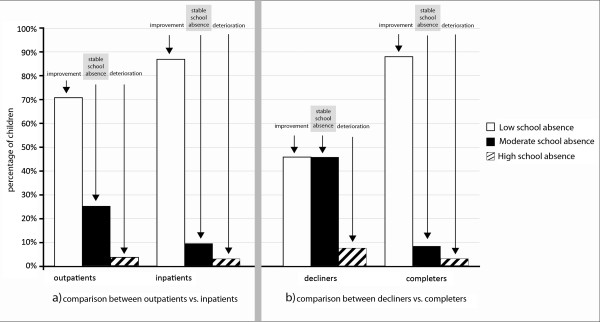
Results: In analysis A, outpatients and inpatients reported comparably low levels of pain intensity (NRS 0-10; mean = 4, SD = 2.7) and disability (Paediatric Pain Disability Index (PPDI: 12-60; mean = 24; SD = 10) at the return visit. Compared to outpatients, more inpatients achieved clinically significant changes in pain intensity (52% vs. 45%) and disability (46% vs. 31%). There were also significantly greater changes in disability in the inpatient group (change score outpatients = 1.0; change score inpatients = 1.4; F(1,1138) = 12.6, p = .011). School absence was substantially reduced, with approximately 80% in each group attending school regularly. Analysis B showed that even though inpatient decliners achieved improvements in the outcome domains, they reported greater disability at the return visit (PPDI mean decliners = 27, SD = 9.9; PPDI mean completers = 24, SD = 10) because they had achieved fewer changes in disability (change score decliners = 0.9; change score completers = 1.4; F(1.334) = 5.7, p = .017). In addition, less decliners than completers achieved clinically significant changes in disability (25% vs. 47%).
Conclusions: Inpatient and outpatient treatments are able to elicit substantial changes in pain intensity, disability and school absence. The results highlight the necessity of intensive inpatient pain treatment for highly affected children, as children who declined inpatient treatment and were treated as outpatients did less well.
Figures
References
-
- Zernikow B, Wager J, Hechler T, Hasan C, Rohr U, Dobe M, Meyer A, Hübner-Möhler B, Wamsler C, Blankenburg M. Characteristics of highly impaired children with severe chronic pain: a 5-year retrospective study on 2249 pediatric pain patients. BMC Pediatr. 2012;12:1–12. doi: 10.1186/1471-2431-12-54. - DOI - PMC - PubMed
-
- Ho IK, Goldschneider KR, Kashikar-Zuck S, Kotagal U, Tessman C, Jones B. Healthcare utilization and indirect burden among families of pediatric patients with chronic pain. J Musculoskelet Pain. 2008;16:155–164. doi: 10.1080/10582450802161853. - DOI
Pre-publication history
-
- The pre-publication history for this paper can be accessed here:http://www.biomedcentral.com/1471-2431/14/262/prepub
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
