

Atrial tachycardias following atrial fibrillation ablation
- PMID: 25308808
- PMCID: PMC4356722
- DOI: 10.2174/1573403x10666141013122400
Atrial tachycardias following atrial fibrillation ablation
Abstract
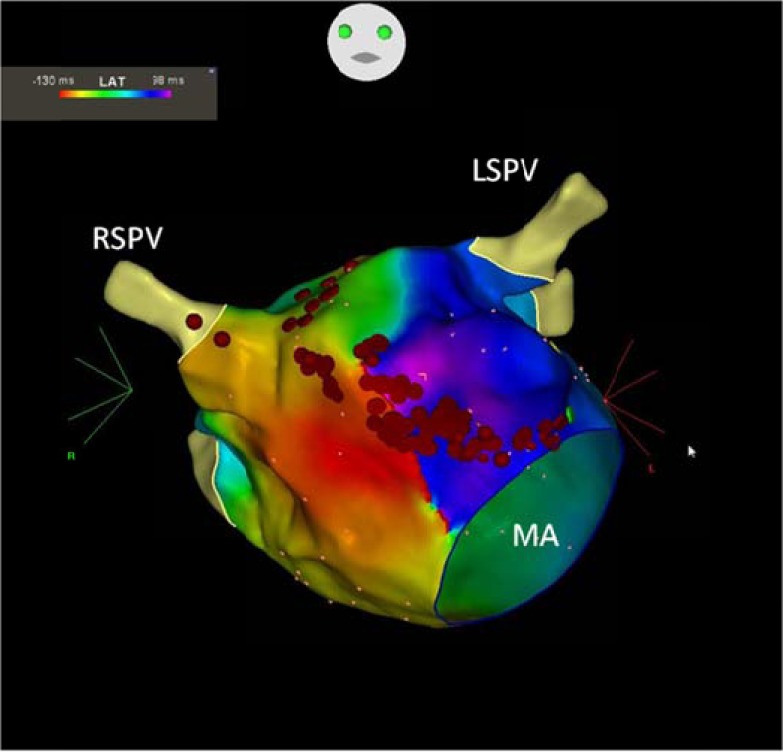
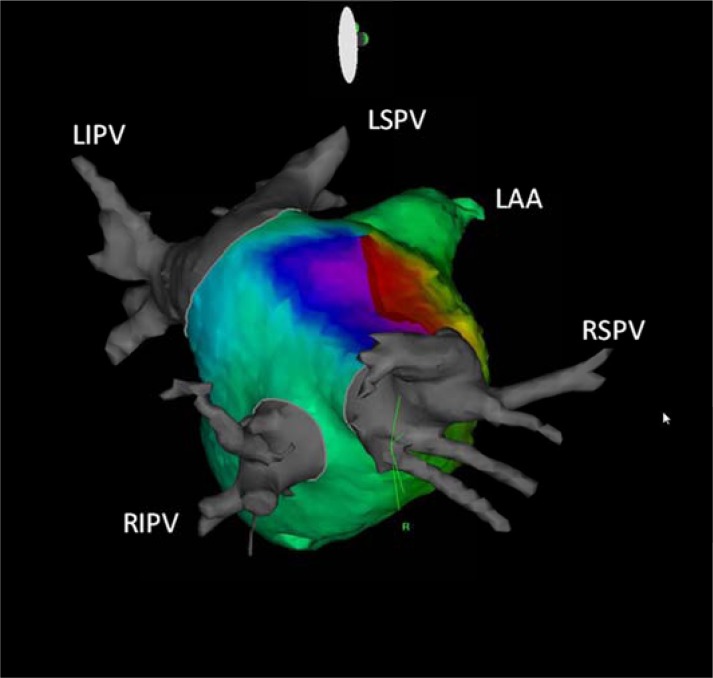
One of the most important proarrhythmic complications after left atrial (LA) ablation is regular atrial tachycardia (AT) or flutter. Those tachycardias that occur after atrial fibrillation (AF) ablation can cause even more severe symptoms than those from the original arrhythmia prior to the index ablation procedure since they are often incessant and associated with rapid ventricular response. Depending on the method and extent of LA ablation and on the electrophysiological properties of underlying LA substrate, the reported incidence of late ATs is variable. To establish the exact mechanism of these tachycardias can be difficult and controversial but correlates with the ablation technique and in the vast majority of cases the mechanism is reentry related to gaps in prior ablation lines. When tachycardias occur, conservative therapy usually is not effective, radiofrequency ablation procedure is mostly successful, but can be challenging, and requires a complex approach.
Figures
References
-
- Oral H, Knight BP, Tada H , et al. Pulmonary vein isolation for paroxysmal and persistent atrial fibrillation. Circulation. 2002;105:1077–81. - PubMed
-
- Oral H, Knight BP, Morady F. Left atrial flutter after segmental ostial radiofrequency catheter ablation for pulmonary vein isolation. Pacing Clin Electrophysiol. 2003;26:1417–9. - PubMed
-
- Gerstenfeld EP, Callans DJ, Dixit S , et al. Mechanisms of organized left atrial tachycardias occurring after pulmonary vein isolation. Circulation. 2004;110:1351–7. - PubMed
-
- Oral H, Scharf C, Chugh A , et al. Catheter ablation for paroxysmal atrial fibrillation Segmental pulmonary vein ostial ablation versus left atrial ablation. Circulation. 2003;108:2355–60. - PubMed
-
- Gaita F, Caponi D, Scaglione M , et al. Long-term clinical results of 2 different ablation strategies in patients with paroxysmal and persistent atrial fibrillation. Circ Arrhythmia Electrophysiol. 2008;1:269–75. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
