

Current Developments and Perspectives on the Diagnosis and Treatment of Urinary Incontinence and Genital Prolapse in Women
- PMID: 25308980
- PMCID: PMC4168362
- DOI: 10.1055/s-0031-1298335
Current Developments and Perspectives on the Diagnosis and Treatment of Urinary Incontinence and Genital Prolapse in Women
Abstract
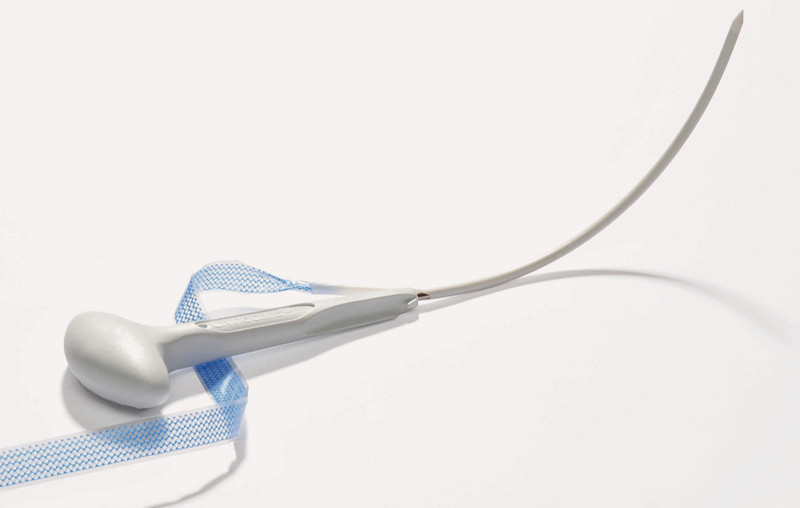
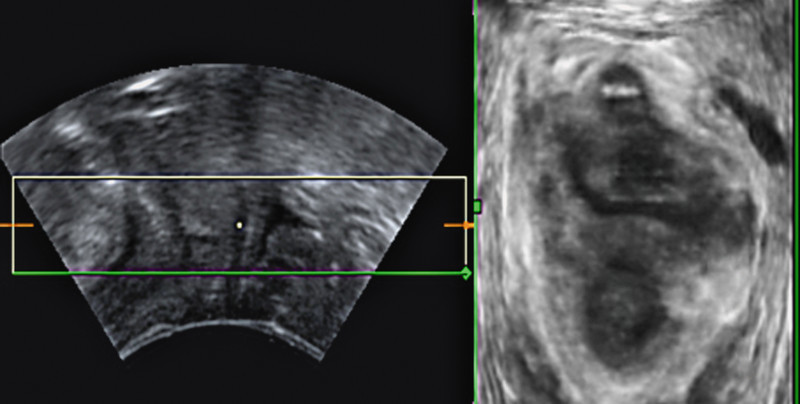
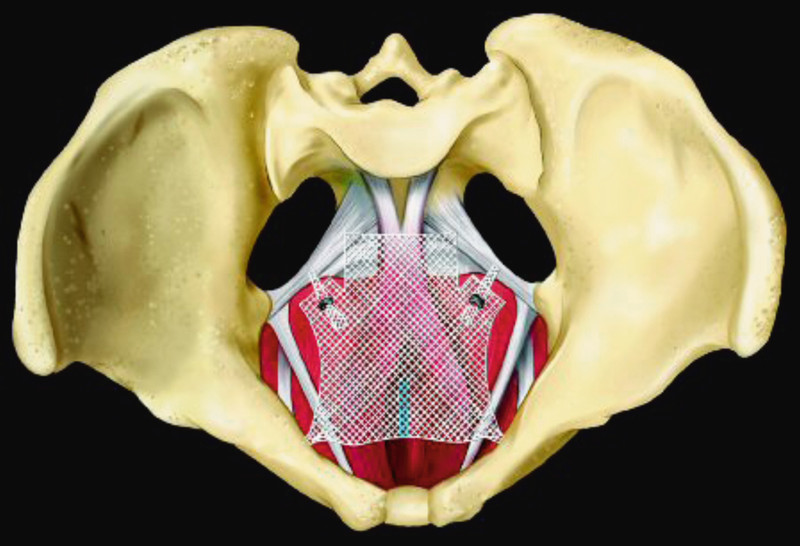
As a key area of gynaecology, urogynaecology has undergone impressive changes in the past few years. Together with the high prevalence of functional pelvic floor disorders, modern anaesthesia procedures and the introduction of new, innovative minimally invasive operation techniques have led to a dramatic increase in the number of operations for incontinence and prolapses. The increasingly subtle diagnostic options, such as, e. g., 2D and 3D sonography of the pelvic floor provide unambiguous findings and facilitate decision making. Tension-free vaginal slings in retro-pubic, trans-obturator or single-incision techniques show a high success rate with few complications and have almost completely replaced the more invasive abdominal surgical techniques for the operative management of stress incontinence. Especially for recurrent prolapse the use of alloplastic nets leads to a markedly improved anatomic and functional outcome. In spite of the euphoria about modern operation techniques and novel net materials, in-depth knowledge of pelvic floor anatomy, sufficient surgical experience and unequivocal guideline-conform indications are mandatory for satisfactory treatment outcomes. The afflicted women must be informed in detail about alternative procedures and more emphasis should be placed on conservative therapy. Novel surgical techniques should be monitored by registers or clinical trials. The professional society is called upon to improve the training curricula for pelvic floor surgery.
Die Urogynäkologie hat sich als große Säule unseres Faches in den letzten Jahren eindrucksvoll verändert. Bei einer hohen Prävalenz an Beckenboden-Funktionsstörungen ist es durch moderne sichere Anästhesieverfahren und Einführung neuer innovativer minimalinvasiver OP-Verfahren zu einem rasanten Zuwachs an Inkontinenz- und Senkungsoperationen gekommen. Immer subtilere diagnostische Möglichkeiten wie z.B. die 2-D- und 3-D-Beckenbodensonografie erbringen klare Befunde zur besseren Entscheidungsfindung. Spannungsfreie Vaginalschlingen in retropubischer, transobturatorischer oder Single-Incision-Technik zeigen hohe Erfolgsraten bei geringen Komplikationen und haben die invasiveren abdominalen Techniken bei der operativen Behandlung der Belastungsinkontinenz weitestgehend abgelöst. Der Einsatz von alloplastischen Meshes führt gerade beim Rezidivprolaps zu einer deutlichen Verbesserung des anatomischen und funktionellen Outcomes. Bei aller Euphorie über moderne Operationstechniken und neue Netzmaterialien sind die profunde Kenntnis der Beckenbodenanatomie, eine ausreichende operative Expertise und eine klare leitliniengerechte Indikationsstellung unverzichtbar für einen zufriedenstellenden Behandlungserfolg. Betroffene Frauen müssen umfassender auch über alternative Verfahren aufgeklärt werden und der konservativen Therapie muss ein größerer Stellenwert gegeben werden. Neue Operationstechniken sollten durch Studien oder Register überwacht werden. Die Fachgesellschaft ist aufgerufen, die Ausbildung des Beckenbodenchirurgen zu verbessern.
Keywords: aconuresis; descensus; urogynecology.
Conflict of interest statement
Figures

References
-
- McKenzie P, Rohozinski J, Badlani G. Genetic influences on stress urinary incontinence. Review. Curr Opin Urol. 2010;20:291–295. - PubMed
-
- Nilsson C G, Palva K, Rezapour M. et al. Eleven years prospective follow-up of the tension-free vaginal tape procedure for treatment of stress urinary incontinence. Int Urogynecol J Pelvic Floor Dysfunction. 2008;19:1043–1047. - PubMed
-
- Ward K L, Hilton P. UK and Ireland TVT Trial Group . Tension-free vaginal tape versus colposuspension for primary urodynamic stress incontinence: 5-year follow up. BJOG. 2008;115:226–233. - PubMed
-
- Latthe P M, Foon R, Toozs-Hobson P. Transobturator and retropubic tape procedures in stress urinary incontinence: a systematic review and meta-analysis of effectiveness and complications. BJOG. 2007;114:522–531. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous