

Severity of nonalcoholic fatty liver disease and progression to cirrhosis are associated with atherogenic lipoprotein profile
- PMID: 25311381
- PMCID: PMC4395517
- DOI: 10.1016/j.cgh.2014.10.008
Severity of nonalcoholic fatty liver disease and progression to cirrhosis are associated with atherogenic lipoprotein profile
Abstract
Background & aims: Nonalcoholic fatty liver disease (NAFLD) is associated independently with increased cardiovascular mortality. Although NAFLD is associated with dyslipidemia, it is not clear whether recently identified markers of cardiovascular risk indicate liver disease progression in patients with histologically confirmed NAFLD. We evaluated an extensive panel of serum markers of cardiovascular risk in nondiabetic patients with histologically proven NAFLD.
Methods: We performed a case-control study in which we compared serum levels of laboratory markers of cardiovascular risk among 81 nondiabetic subjects with histologically confirmed NAFLD vs lean (N = 81) and obese (N = 81) individuals without NAFLD (based on liver fat score, controls). For ex vivo studies, liver tissues were obtained from subjects undergoing elective cholecystectomy or from a tissue repository.
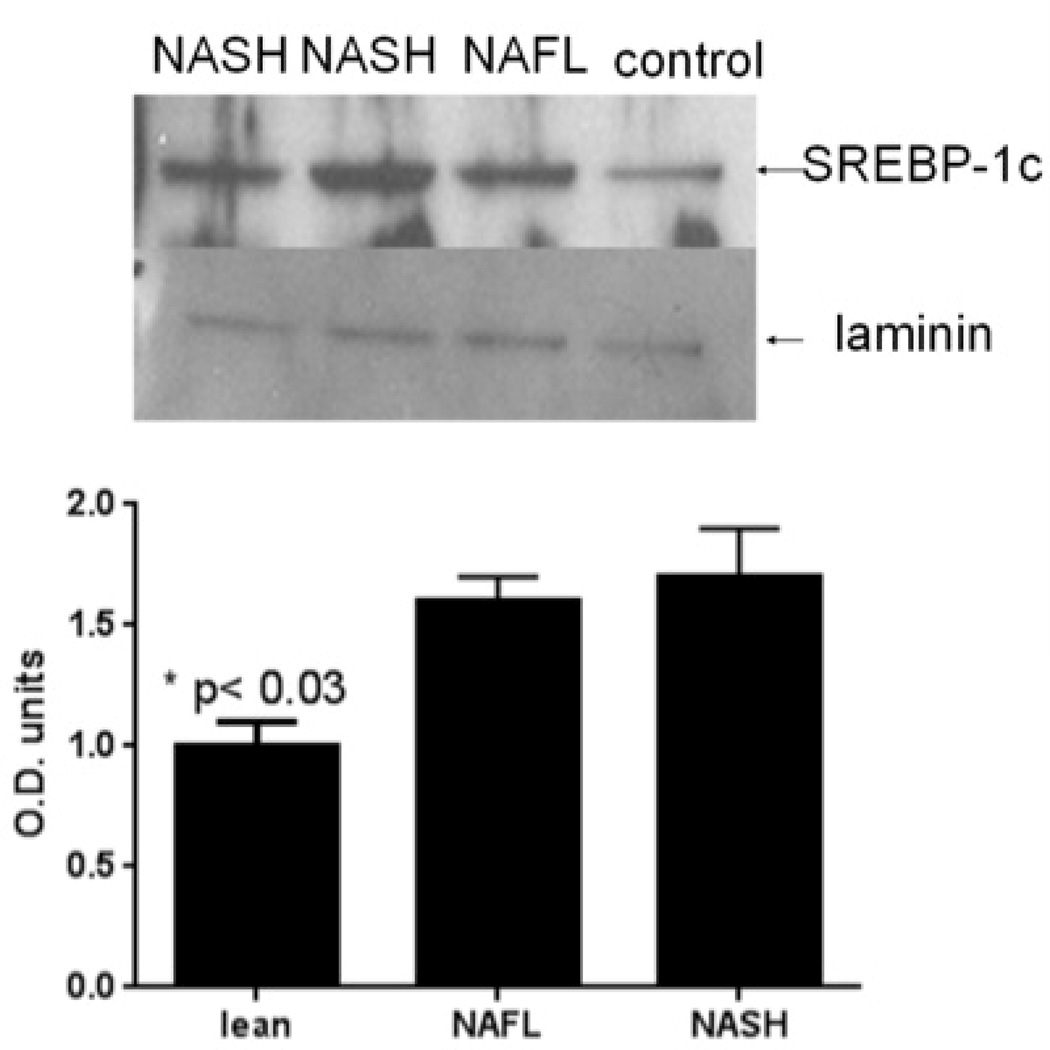
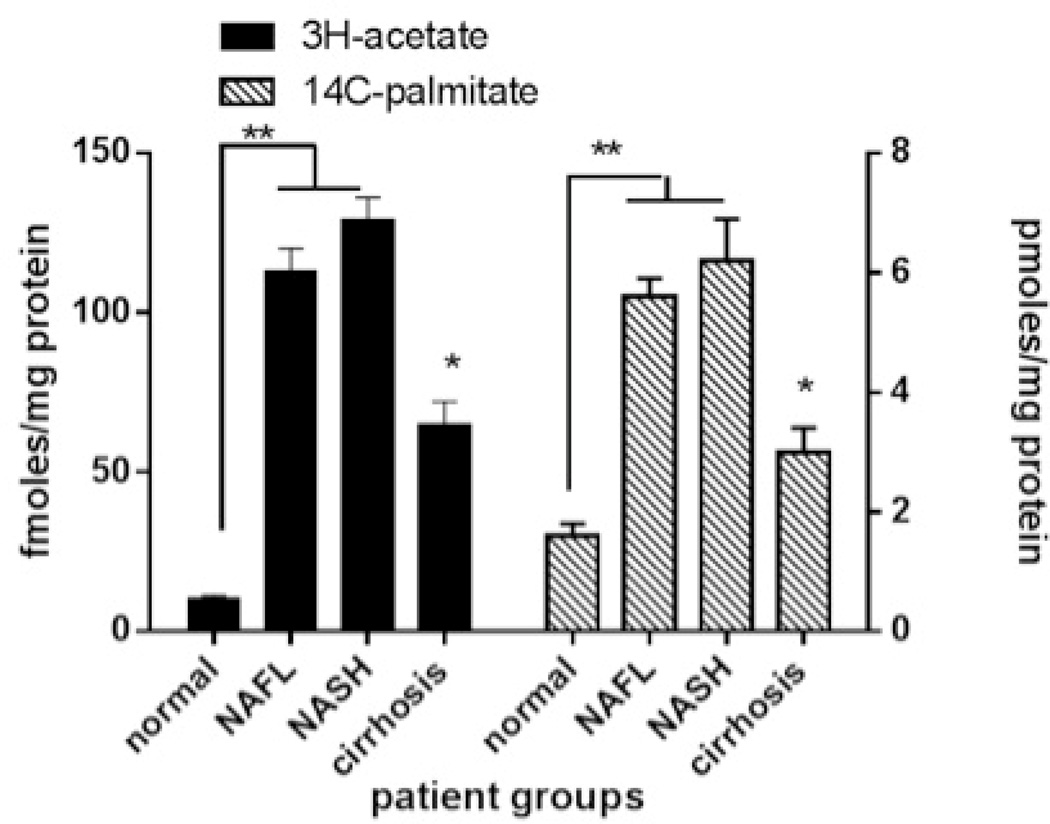
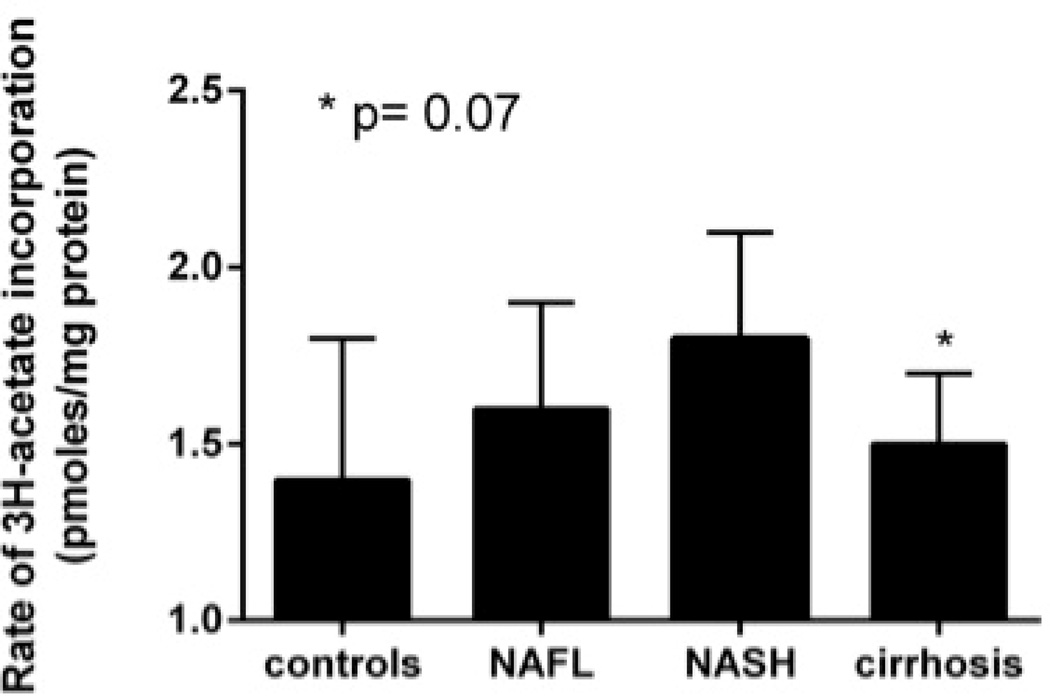
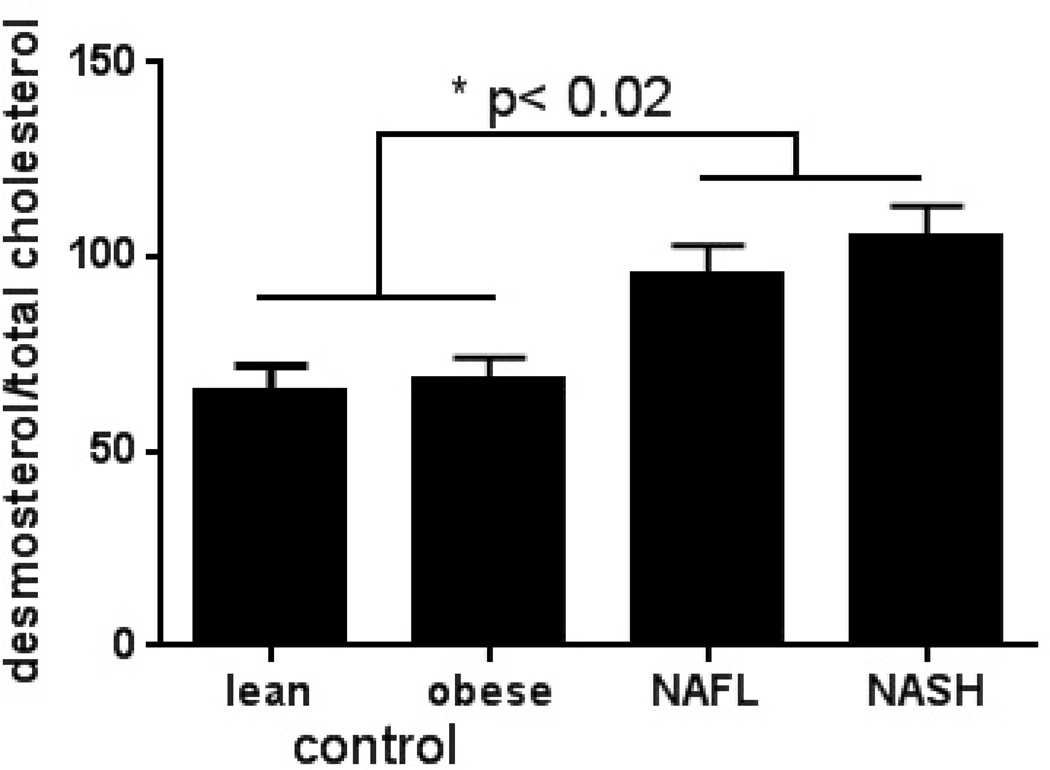
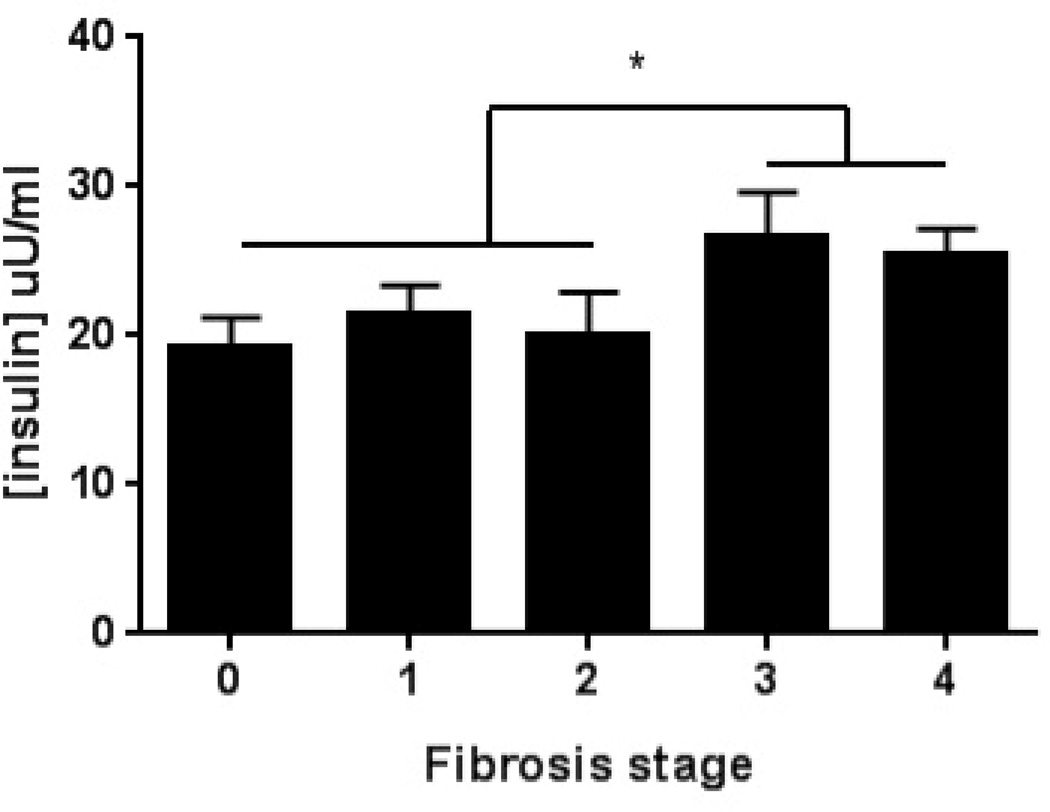
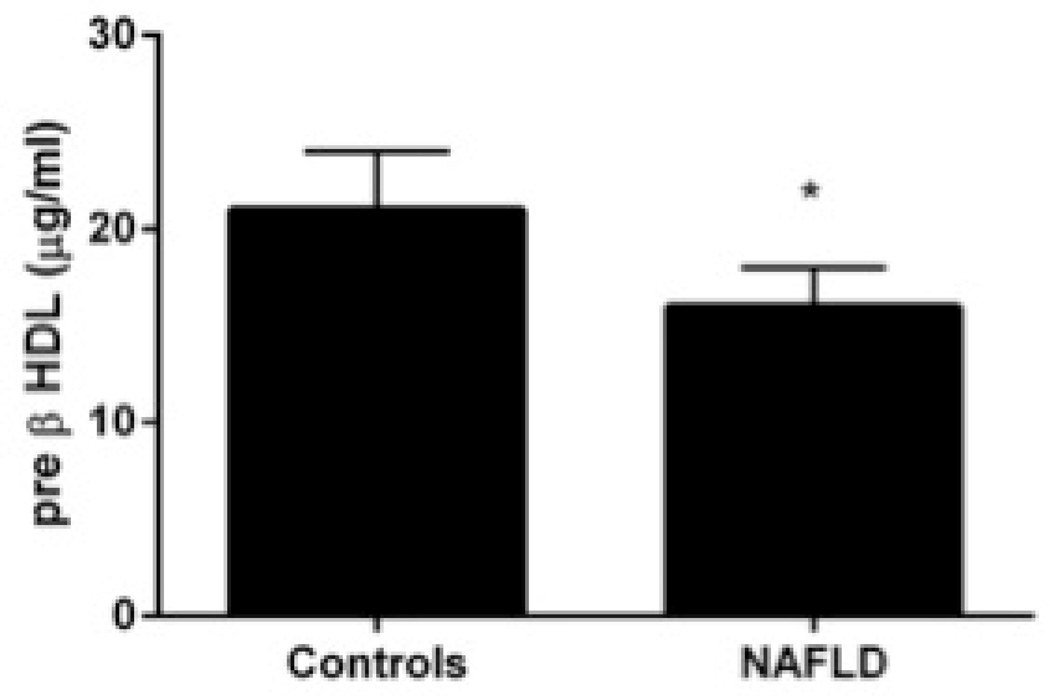
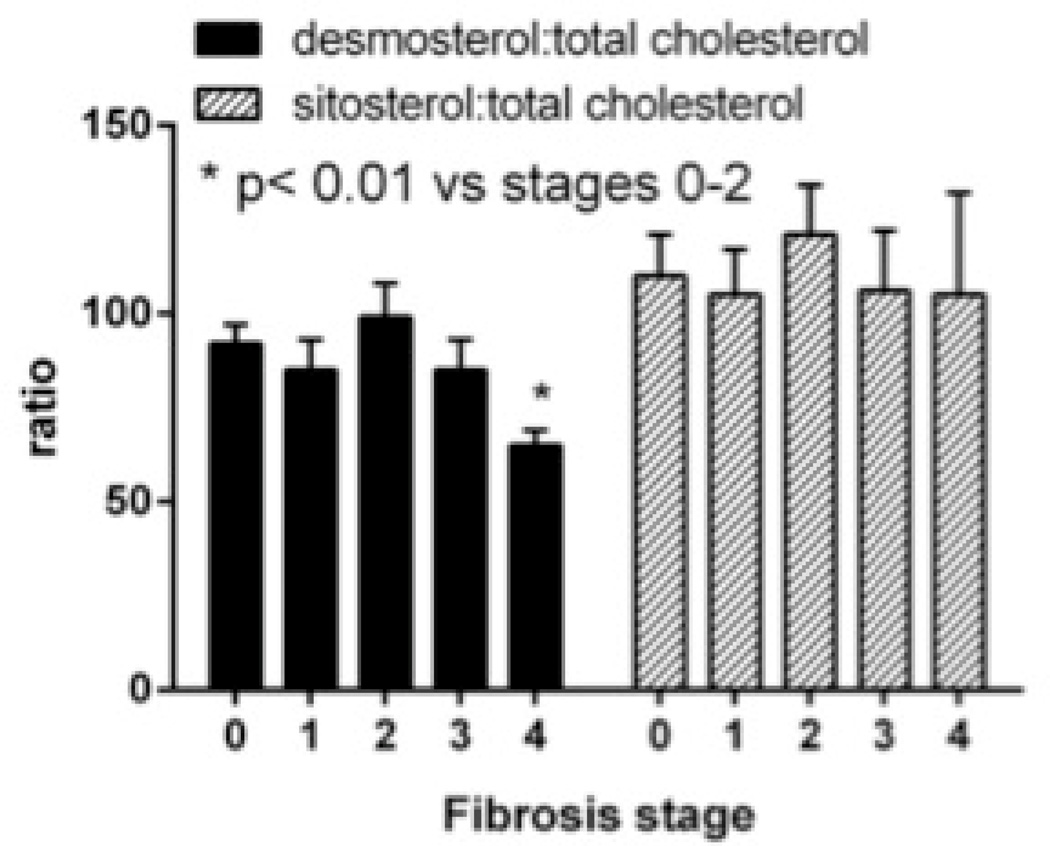
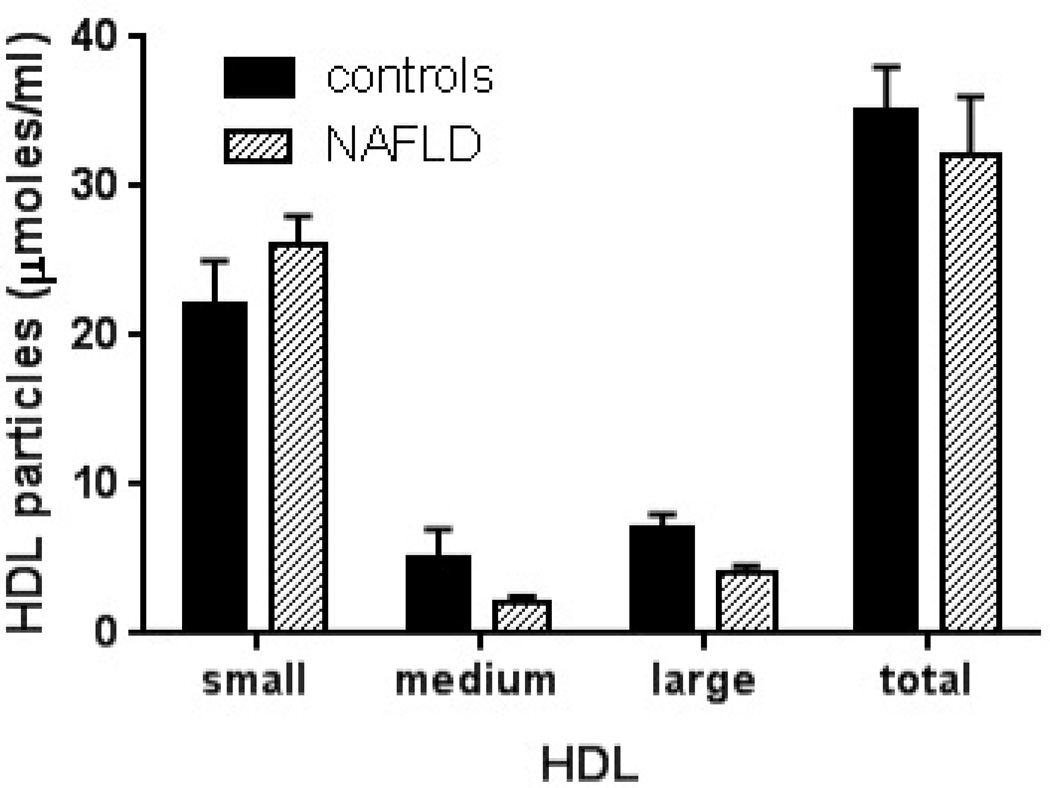
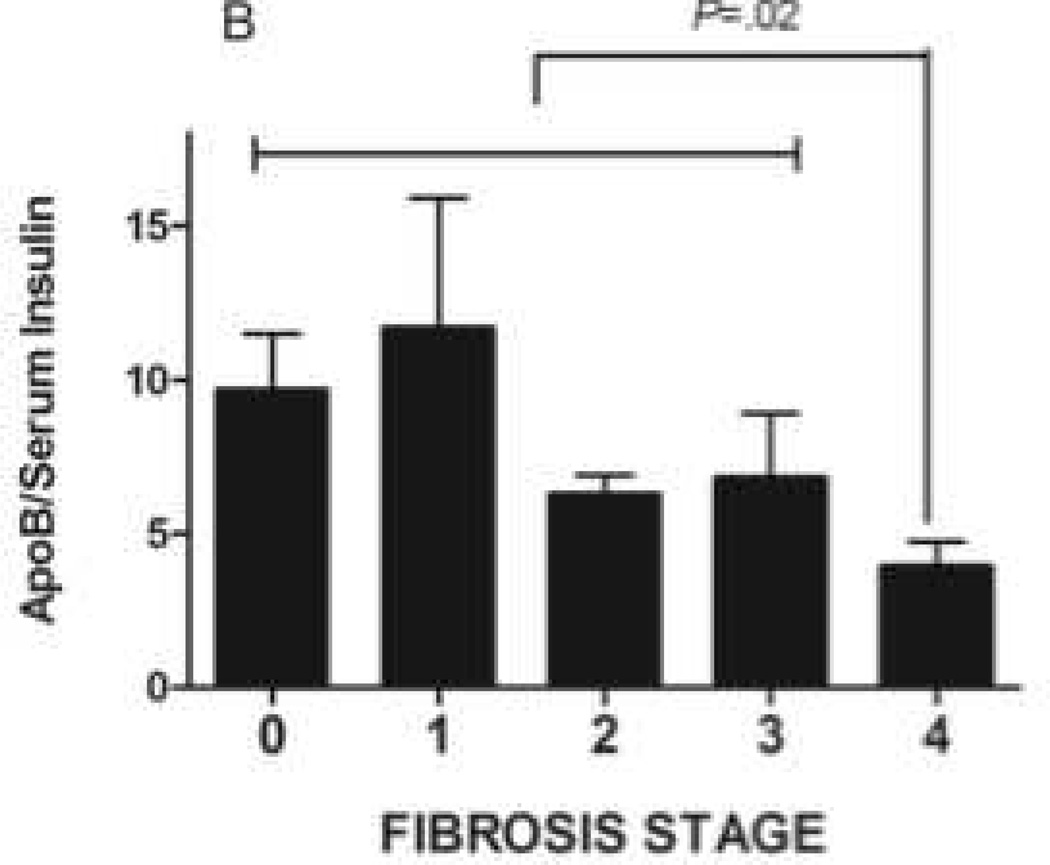
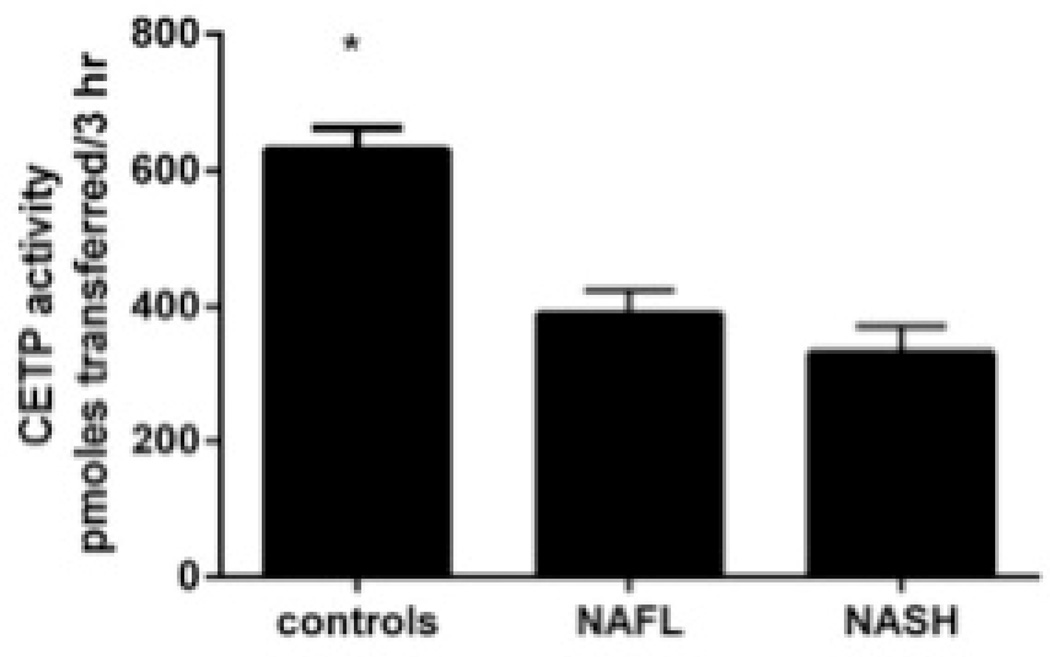
Results: Subjects with NAFLD had increased serum levels of insulin, triglycerides, and apolipoprotein B; increased size and concentration of very large density lipoprotein particles; increased concentrations of low-density lipoprotein (LDL) particles and small dense LDL (sdLDL) cholesterol, and an increased percentage of sdLDL, compared with controls. Although nonalcoholic steatohepatitis was associated with a worse profile of serum atherogenic markers than NAFLD, these differences did not reach statistical significance. Despite hyperinsulinemia, triglyceride and apolipoprotein B levels, concentrations of LDL particles and LDL cholesterol, and sdLDL-related parameters decreased significantly in patients with cirrhosis. Ex vivo studies showed that patients with NAFLD had increased sensitivity of hepatic triglyceride levels and cholesterol synthesis to insulin, and that sensitivity increased the development of cirrhosis.
Conclusions: Atherogenic dyslipidemia is related to increased insulin-induced hepatic lipid synthesis in patients with NAFLD. Reduced dyslipidemia in patients with cirrhosis is associated with increased insulin resistance and possibly failed lipid synthesis.
Keywords: Heart Disease; Metabolic Syndrome; NASH; Obesity; Steatosis.
Copyright © 2015 AGA Institute. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Figures
References
-
- Vernon G, Baranova A, Younossi ZM. Systematic review: the epidemiology and natural history of non-alcoholic fatty liver disease and non-alcholic steatohepatitis in adults. Hepatology. 2011;34:274–285. - PubMed
-
- Chalasani N, Younossi Z, Lavine JE, et al. The diagnosis and management of non-alcoholic fatty liver disease: Practice guideline by the american association for the study of liver diseases, American College of Gastroenterology, and the American Gastroenterological Association. Hepatology. 2012;55:n/a–n/a. - PubMed
-
- Adams LA, Lymp JF, St Sauver J, et al. The natural history of nonalcoholic fatty liver disease: a population-based cohort study. Gastroenterology. 2005;129:113–121. - PubMed
-
- Targher G, Day CP, Bonora E. Risk of cardiovascular disease in patients with nonalcoholic fatty liver disease. N Engl J Med. 2010;363:1341–1350. - PubMed
-
- Herder C, Karakas M, Koenig W. Biomarkers for the Prediction of Type 2 Diabetes and Cardiovascular Disease. Clinical Pharmacology & Therapeutics. 2011;90:52–66. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
