

Tumour responses following a steroid switch from prednisone to dexamethasone in castration-resistant prostate cancer patients progressing on abiraterone
- PMID: 25314055
- PMCID: PMC4264443
- DOI: 10.1038/bjc.2014.531
Tumour responses following a steroid switch from prednisone to dexamethasone in castration-resistant prostate cancer patients progressing on abiraterone
Abstract
Background: Abiraterone is a CYP17A1 inhibitor that improves survival in castration-resistant prostate cancer (CRPC). Abiraterone is licensed in combination with prednisone 5 mg twice daily to prevent a syndrome of secondary mineralocorticoid excess. We hypothesised that a 'steroid switch' from prednisone to dexamethasone would induce secondary responses in patients progressing on abiraterone and prednisone 5 mg b.i.d.
Methods: We performed a 'steroid switch' in patients with CRPC at PSA progression on abiraterone and prednisolone. Patients were monitored for secondary declines in PSA, radiological tumour regression and toxicity.
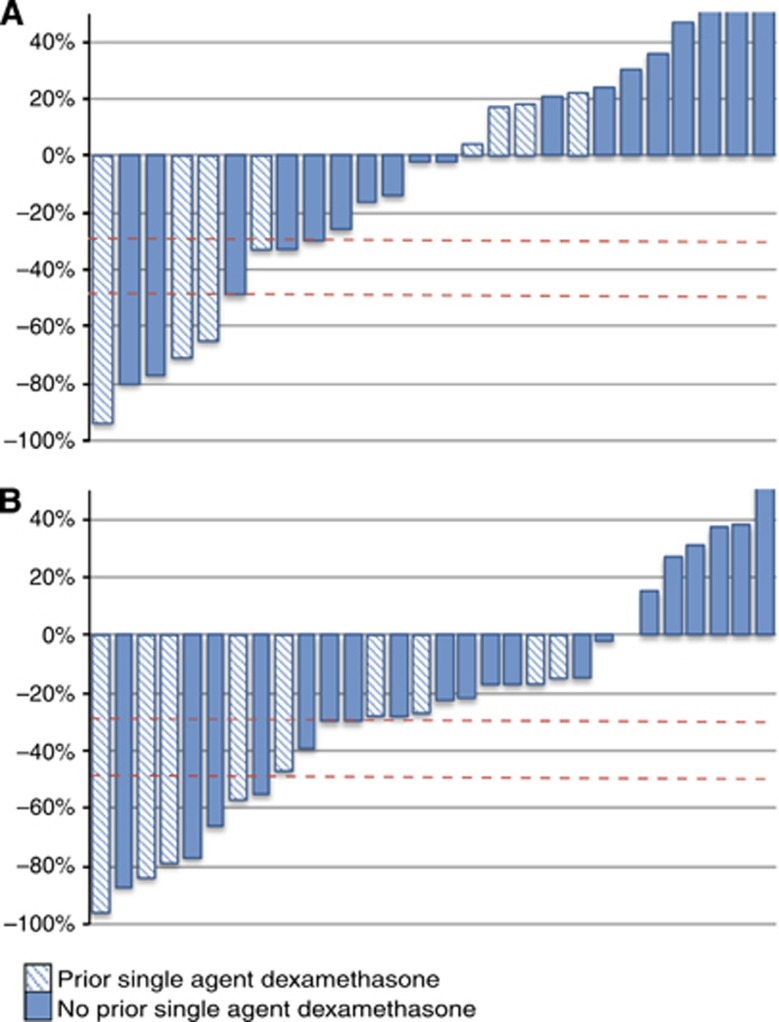
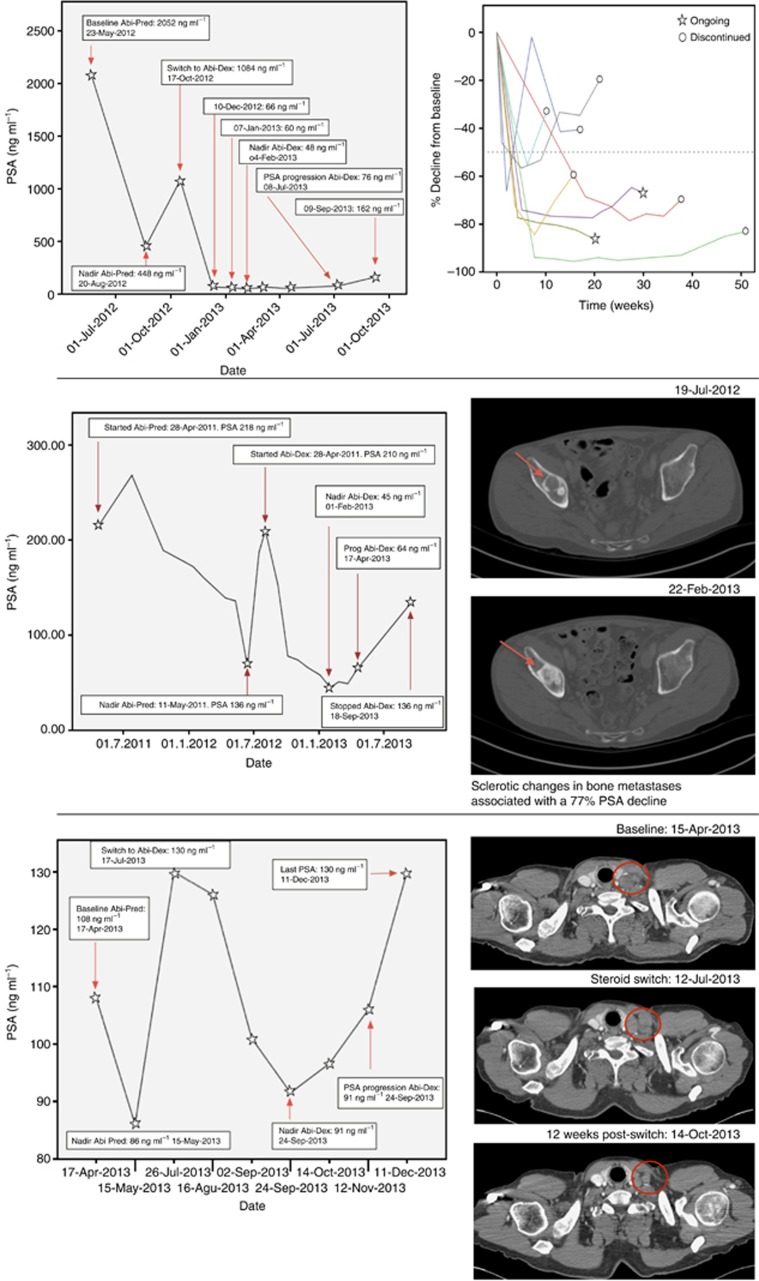
Results: A retrospective analysis of 30 CRPC patients who underwent a steroid switch from prednisolone to dexamethasone while on abiraterone was performed. A total of six patients (20%) had a ⩾50% PSA decline that was confirmed by a second PSA level at least 3 weeks later. In all, 11 patients (39.2%) had a confirmed ⩾30% PSA decline. Median time to PSA progression on abiraterone and dexamethasone was 11.7 weeks (95% CI: 8.6-14.8 weeks) in the whole cohort and 27.6 weeks (95% CI: 14.5-40.7 weeks) in patients who achieved a confirmed 50% PSA decline. Nine patients had RECIST evaluable disease: two of these patients had RECIST partial response, six patients had stable disease and one patient had progressive disease at the first imaging assessment. Treatment was well tolerated, with no grade 3 and grade 4 adverse events. One patient had to be reverted to prednisolone because of grade 2 hypotension.
Conclusions: Durable PSA responses occur in up to 40% of patients following a 'steroid switch' for PSA progression on abiraterone and prednisone. Studies are ongoing to elucidate the mechanisms underlying this response.
Figures
References
-
- Attard G, Reid AH, A'Hern R, Parker C, Oommen NB, Folkerd E, Messiou C, Molife LR, Maier G, Thompson E, Olmos D, Sinha R, Lee G, Dowsett M, Kaye SB, Dearnaley D, Kheoh T, Molina A, de Bono JS. Selective inhibition of CYP17 with abiraterone acetate is highly active in the treatment of castration-resistant prostate cancer. J Clin Oncol. 2009;27 (23:3742–3748. - PMC - PubMed
-
- Attard G, Reid AH, Yap TA, Raynaud F, Dowsett M, Settatree S, Barrett M, Parker C, Martins V, Folkerd E, Clark J, Cooper CS, Kaye SB, Dearnaley D, Lee G, de Bono JS. Phase i clinical trial of a selective inhibitor of CYP17, abiraterone acetate, confirms that castration-resistant prostate cancer commonly remains hormone driven. J Clinical Oncology: Official Journal of the American Society of Clinical Oncology. 2008;26 (28:4563–4571. - PubMed
-
- Beheshti M, Vali R, Waldenberger P, Fitz F, Nader M, Loidl W, Broinger G, Stoiber F, Foglman I, Langsteger W. Detection of bone metastases in patients with prostate cancer by 18F fluorocholine and 18F fluoride PET-CT: a comparative study. Eur J Nucl Med Mol Imaging. 2008;35 (10:1766–1774. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
