

Diagnostic delays and clinical decision making with centralized Xpert MTB/RIF testing in Durban, South Africa
- PMID: 25314255
- PMCID: PMC4197409
- DOI: 10.1097/QAI.0000000000000309
Diagnostic delays and clinical decision making with centralized Xpert MTB/RIF testing in Durban, South Africa
Abstract
Setting: We conducted a retrospective study among HIV-infected adult suspects (≥18 years) with pulmonary tuberculosis (TB), who underwent Xpert MTB/RIF (Xpert) testing at McCord Hospital and its adjoining HIV clinic in Durban, South Africa.
Objective: To determine if Xpert testing performed at a centralized laboratory accelerated time to TB diagnosis.
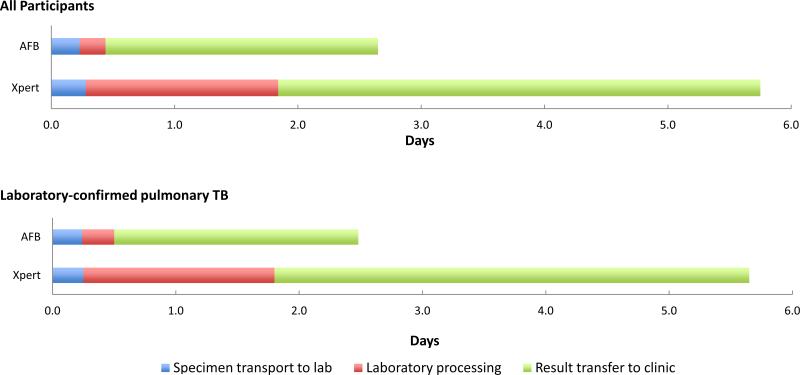
Design: We obtained data on sputum smear microscopy [acid-fast bacilli (AFB)], Xpert, and the rationale for treatment initiation from medical records. The primary outcome was "total diagnostic time," defined as time from sputum collection to clinicians' receipt of results. A linear mixed-effect model compared the duration of steps in the diagnostic pathway across testing modalities.
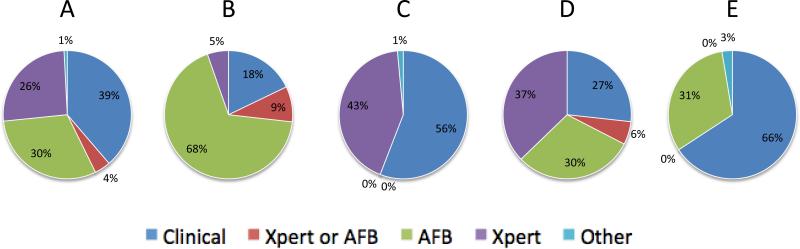
Results: Among 403 participants, the median "total diagnostic time" for AFB and Xpert was 3.3 and 6.4 days, respectively (P < 0.001). When compared with AFB, the median delay for Xpert "laboratory processing" was 1.4 days (P < 0.001) and "result transfer to clinic" was 1.7 days (P < 0.001). Among 86 Xpert-positive participants who initiated treatment, 49 (57%) started treatment based on clinical suspicion or AFB-positive results, whereas only 32 (37%) started treatment based on Xpert-positive results.
Conclusions: In our setting, Xpert results took twice as long as AFB results to reach clinicians. Replacing AFB with centralized Xpert may delay TB diagnoses in some settings.
Figures
References
-
- World Health Organization (WHO) Global Tuberculosis Control 2011. WHO; Geneva, Switzerland: 2011.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
