

Pituitary apoplexy: an update on clinical and imaging features
- PMID: 25315035
- PMCID: PMC4263799
- DOI: 10.1007/s13244-014-0362-0
Pituitary apoplexy: an update on clinical and imaging features
Abstract
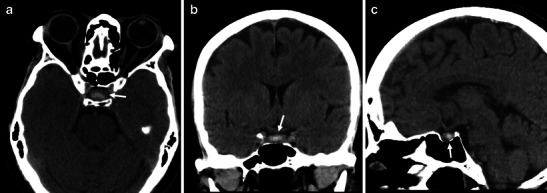
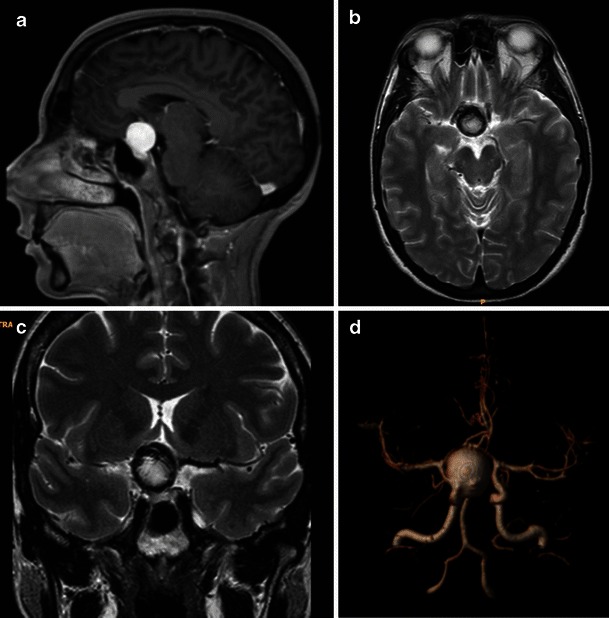
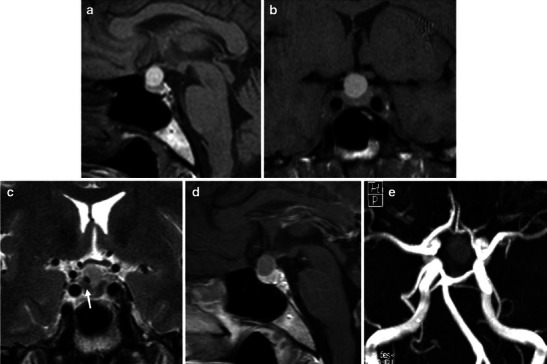
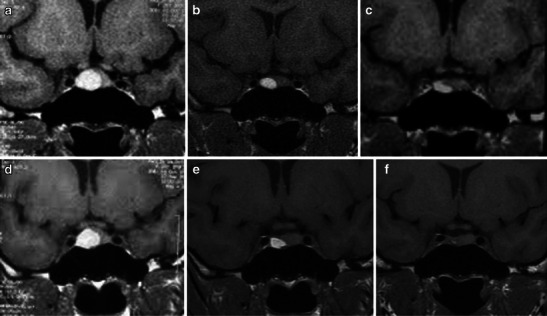
Pituitary apoplexy (PA) is a rare and potentially fatal clinical condition presenting acute headache, vomiting, visual impairment, ophthalmoplegia, altered mental state and possible panhypopituitarism. It mostly occurs in patients with haemorrhagic infarction of the pituitary gland due to a pre-existing macroadenoma. Although there are pathological and physiological conditions that may share similar imaging characteristics, both clinical and imaging features can guide the radiologist towards the correct diagnosis, especially using magnetic resonance imaging (MRI). In this review, we will describe the main clinical and epidemiological features of PA, illustrating CT and MRI findings and discussing the role of imaging in the differential diagnosis, prognosis and follow-up. Teaching points • Headache, ophtalmoplegia and visual impairment are frequent symptoms of pituitary apoplexy. • CT is often the first imaging tool in PA, showing areas of hyperdensity within the sellar region. • MRI could confirm haemorrhage within the pituitary gland and compression on the optic chiasm. • Frequent simulating conditions are aneurysms, Rathke cleft cysts, craniopharingioma and mucocele. • The role of imaging is still debated and needs more studies.
Figures




Similar articles
-
Clinical and imaging features of pituitary apoplexy and role of imaging in differentiation of clinical mimics.Quant Imaging Med Surg. 2018 Mar;8(2):219-231. doi: 10.21037/qims.2018.03.08. Quant Imaging Med Surg. 2018. PMID: 29675363 Free PMC article. Review.
-
Rathke Cleft Cysts with Apoplexy-Like Symptoms: Clinicoradiologic Comparisons with Pituitary Adenomas with Apoplexy.World Neurosurg. 2020 Oct;142:e1-e9. doi: 10.1016/j.wneu.2020.03.086. Epub 2020 Mar 23. World Neurosurg. 2020. PMID: 32217176
-
An altered state of consciousness while using anticoagulants and the incidental discovery of a pituitary lesion: considering pituitary apoplexy.Endocrinol Diabetes Metab Case Rep. 2022 Jun 1;2022:21-0204. doi: 10.1530/EDM-21-0204. Online ahead of print. Endocrinol Diabetes Metab Case Rep. 2022. PMID: 35730462 Free PMC article.
-
Classical pituitary apoplexy: clinical features, management and outcome.Clin Endocrinol (Oxf). 1999 Aug;51(2):181-8. doi: 10.1046/j.1365-2265.1999.00754.x. Clin Endocrinol (Oxf). 1999. PMID: 10468988
-
Presenting Symptoms of Pituitary Apoplexy.J Neurol Surg A Cent Eur Neurosurg. 2018 Jan;79(1):52-59. doi: 10.1055/s-0037-1599051. Epub 2017 Apr 24. J Neurol Surg A Cent Eur Neurosurg. 2018. PMID: 28437813 Review.
Cited by
-
Pituitary apoplexy associated with bacterial meningitis: Diagnostic dilemma.Clin Case Rep. 2023 Sep 3;11(9):e7887. doi: 10.1002/ccr3.7887. eCollection 2023 Sep. Clin Case Rep. 2023. PMID: 37670816 Free PMC article.
-
A Case of Spontaneously Resolving Cushing Disease.JCEM Case Rep. 2025 Jul 10;3(8):luaf131. doi: 10.1210/jcemcr/luaf131. eCollection 2025 Aug. JCEM Case Rep. 2025. PMID: 40642336 Free PMC article.
-
Giant pituitary macroadenoma with apoplexy presenting with isolated bilateral hypoglossal nerve palsy: illustrative case.J Neurosurg Case Lessons. 2024 Sep 30;8(14):CASE24326. doi: 10.3171/CASE24326. Print 2024 Sep 30. J Neurosurg Case Lessons. 2024. PMID: 39348723 Free PMC article.
-
Pilot Findings on SARS-CoV-2 Vaccine-Induced Pituitary Diseases: A Mini Review from Diagnosis to Pathophysiology.Vaccines (Basel). 2022 Nov 24;10(12):2004. doi: 10.3390/vaccines10122004. Vaccines (Basel). 2022. PMID: 36560413 Free PMC article. Review.
-
Atypical teratoid/rhabdoid tumor presenting with subarachnoid and intraventricular hemorrhage.Surg Neurol Int. 2019 Jul 5;10:139. doi: 10.25259/SNI-59-2019. eCollection 2019. Surg Neurol Int. 2019. PMID: 31528474 Free PMC article.
References
-
- Bailey P. Pathological report of a case of acromegaly with special reference to the lesions in hypophysis cerebri and in the thyroid gland, and a case of hemorrhage into the pituitary. Phila Med J. 1898;1:789–792.
LinkOut - more resources
Full Text Sources
Other Literature Sources
