

Validity of acute stroke lesion volume estimation by diffusion-weighted imaging-Alberta Stroke Program Early Computed Tomographic Score depends on lesion location in 496 patients with middle cerebral artery stroke
- PMID: 25316278
- PMCID: PMC4749150
- DOI: 10.1161/STROKEAHA.114.006694
Validity of acute stroke lesion volume estimation by diffusion-weighted imaging-Alberta Stroke Program Early Computed Tomographic Score depends on lesion location in 496 patients with middle cerebral artery stroke
Abstract
Background and purpose: Alberta Stroke Program Early Computed Tomographic Score (ASPECTS) has been used to estimate diffusion-weighted imaging (DWI) lesion volume in acute stroke. We aimed to assess correlations of DWI-ASPECTS with lesion volume in different middle cerebral artery (MCA) subregions and reproduce existing ASPECTS thresholds of a malignant profile defined by lesion volume ≥100 mL.
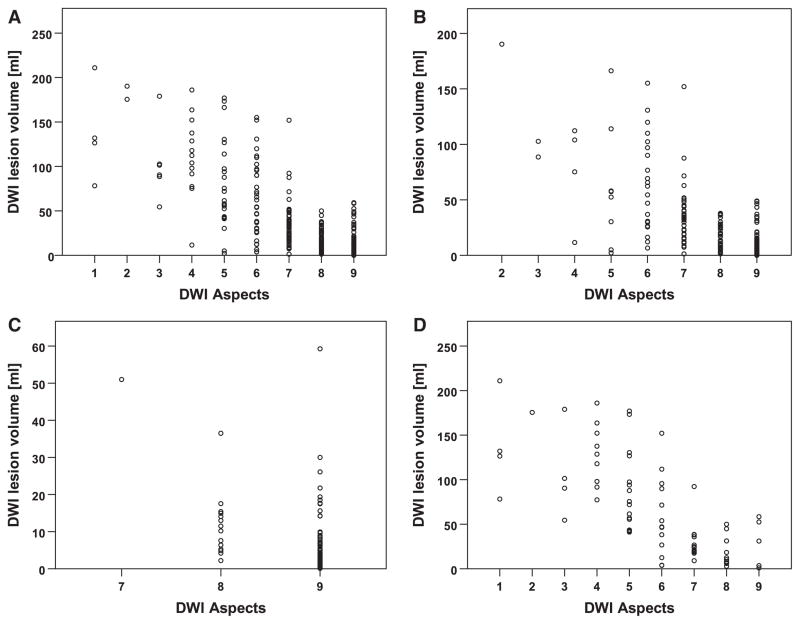
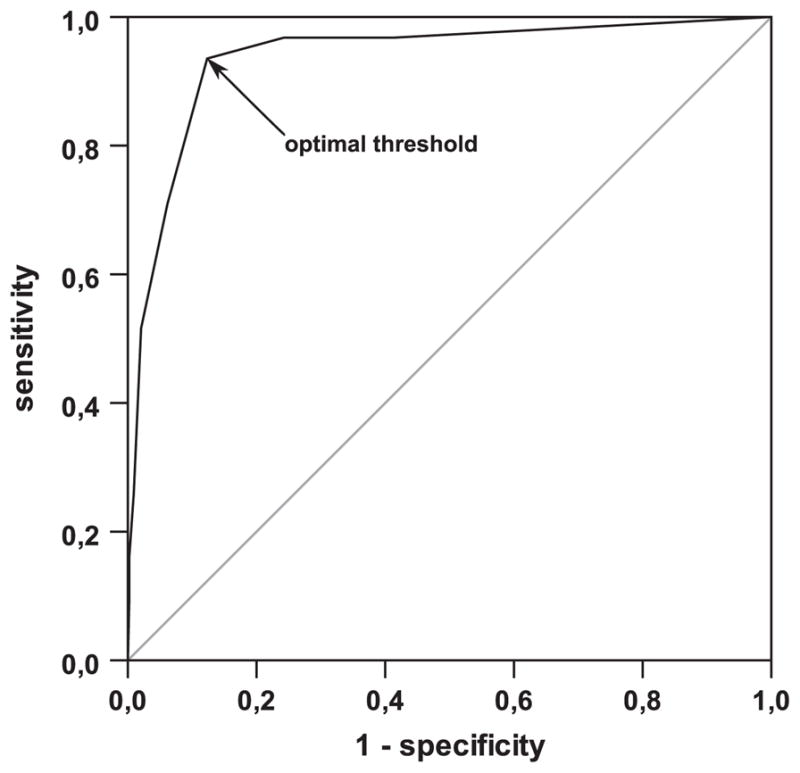
Methods: We analyzed data of patients with MCA stroke from a prospective observational study of DWI and fluid-attenuated inversion recovery in acute stroke. DWI-ASPECTS and lesion volume were calculated. The population was divided into subgroups based on lesion localization (superficial MCA territory, deep MCA territory, or both). Correlation of ASPECTS and infarct volume was calculated, and receiver-operating characteristics curve analysis was performed to identify the optimal ASPECTS threshold for ≥100-mL lesion volume.
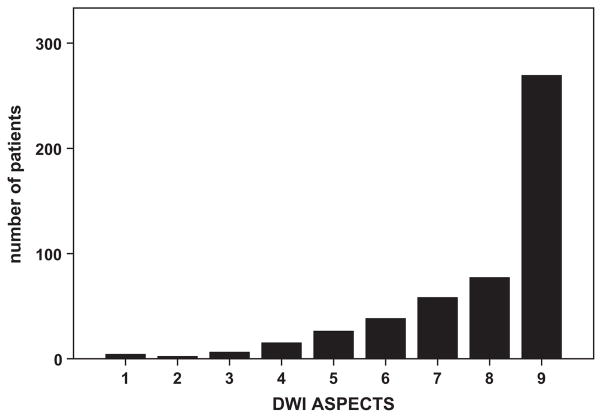
Results: A total of 496 patients were included. There was a significant negative correlation between ASPECTS and DWI lesion volume (r=-0.78; P<0.0001). With regards to lesion localization, correlation was weaker in deep MCA region (r=-0.19; P=0.038) when compared with superficial (r=-0.72; P<0.001) or combined superficial and deep MCA lesions (r=-0.72; P<0.001). Receiver-operating characteristics analysis revealed ASPECTS≤6 as best cutoff to identify ≥100-mL DWI lesion volume; however, positive predictive value was low (0.35).
Conclusions: ASPECTS has limitations when lesion location is not considered. Identification of patients with malignant profile by DWI-ASPECTS may be unreliable. ASPECTS may be a useful tool for the evaluation of noncontrast computed tomography. However, if MRI is used, ASPECTS seems dispensable because lesion volume can easily be quantified on DWI maps.
Keywords: brain ischemia; diffusion magnetic resonance imaging; magnetic resonance imaging; middle cerebral artery; neuroimaging; severity of illness index; stroke.
© 2014 American Heart Association, Inc.
Figures
References
-
- Barber P, Demchuk A, Zhang J, Buchan A. Validity and reliability of a quantitative computed tomography score in predicting outcome of hyperacute stroke before thrombolytic therapy. Lancet. 2000;355:1670–1674. - PubMed
-
- Mitomi M, Kimura K, Aoki J, Iguchi Y. Comparison of CT and DWI findings in ischemic stroke patients within 3 hours of onset. J Stroke Cerebrovasc Dis. 2014;23:37–42. - PubMed
-
- Albers GW, Thijs VN, Wechsler L, Kemp S, Schlaug G, Skalabrin E, et al. Magnetic resonance imaging profiles predict clinical response to early reperfusion: the diffusion and perfusion imaging evaluation for understanding stroke evolution (DEFUSE) study. Ann Neurol. 2006;60:508–517. - PubMed
-
- Singer OC, Kurre W, Humpich MC, Lorenz MW, Kastrup A, Liebeskind DS, et al. Risk assessment of symptomatic intracerebral hemorrhage after thrombolysis using DWI-ASPECTS. Stroke. 2009;40:2743–2748. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
