

Ovarian cystectomy in endometriomas: Combined approach
- PMID: 25317047
- PMCID: PMC4195329
- DOI: 10.5152/jtgga.2014.1111
Ovarian cystectomy in endometriomas: Combined approach
Abstract
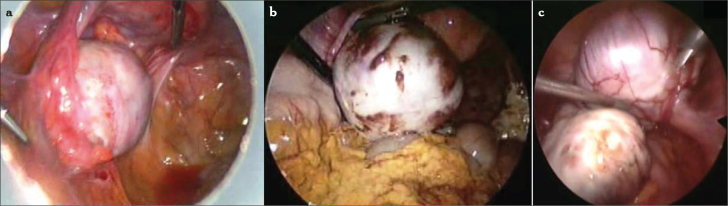
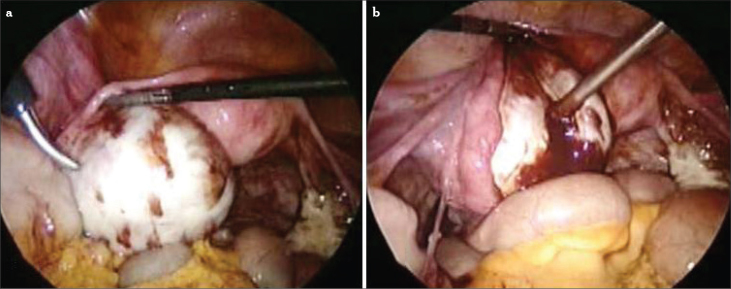
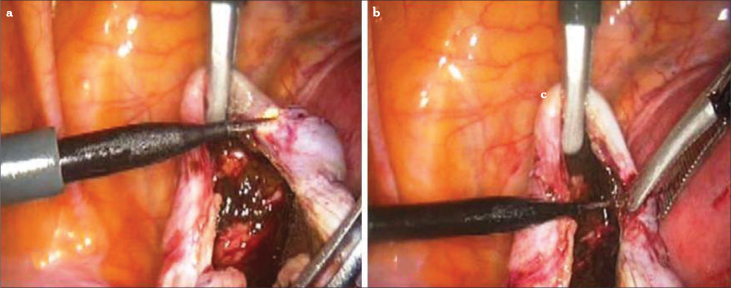
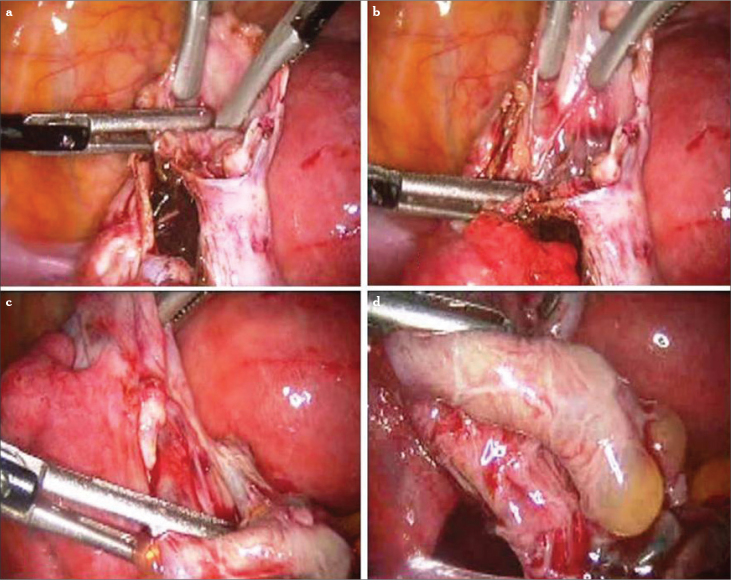
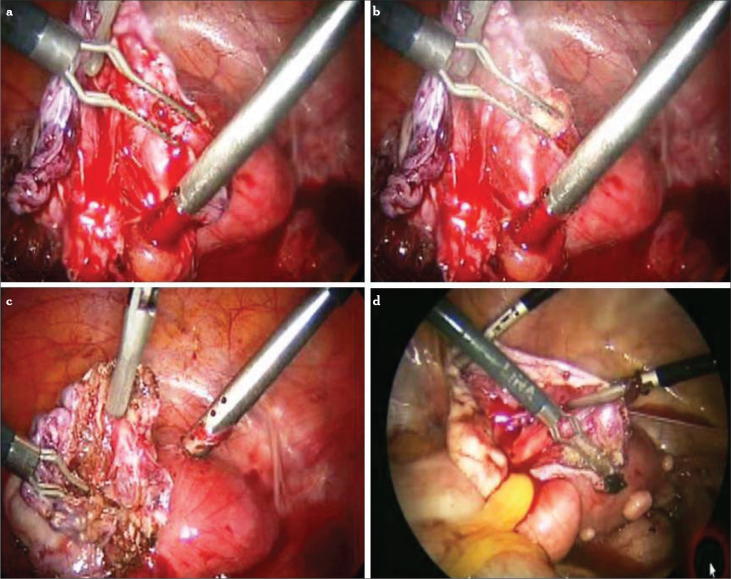
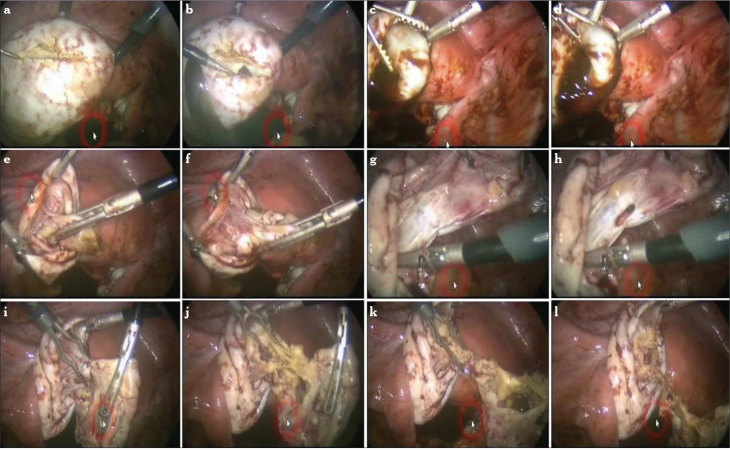
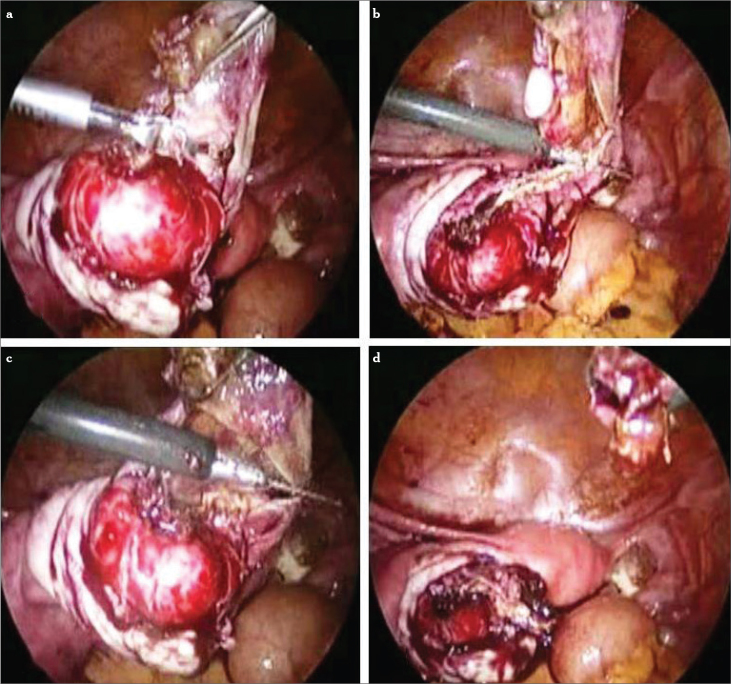
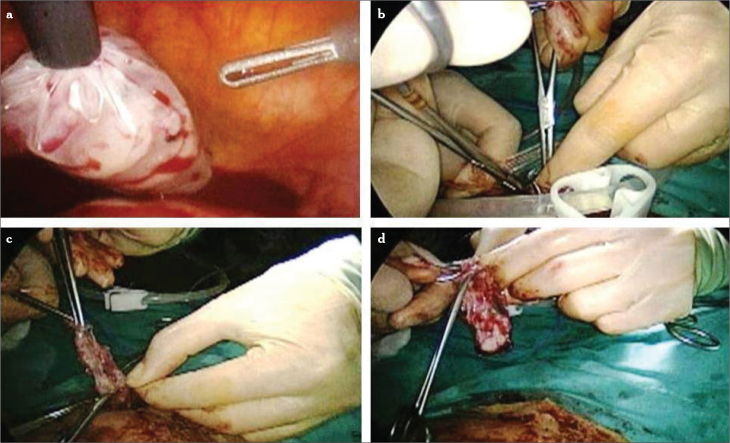
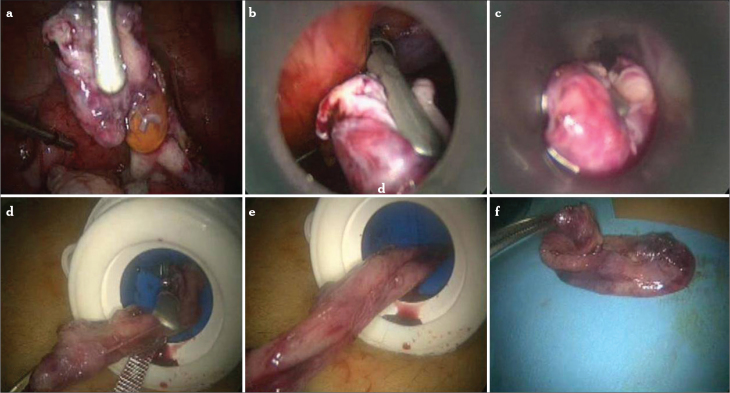
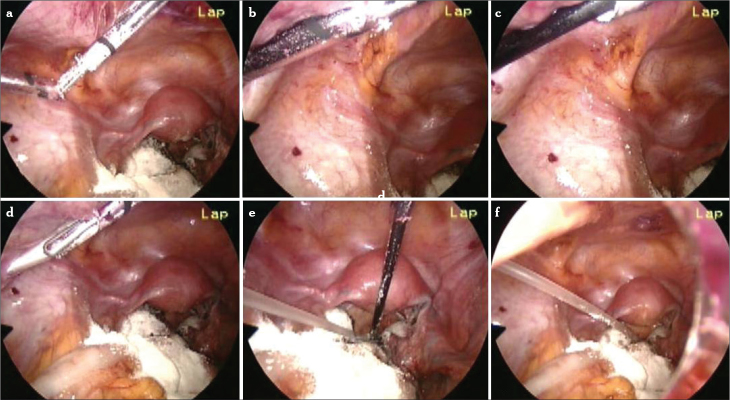
Endometrioma is one of the most frequent adnexal masses in the premenopausal population, but the recommended treatment is still a subject of debate. Medical therapy is inefficient and can not be recommended in the management of ovarian endometriomas. The general consensus is that ovarian endometriomas larger than 4 cm should be removed, both to reduce pain and to improve spontaneous conception rates. The removal of ovarian endometriomas can be difficult, as the capsule is often densely adherent. While the surgical treatment of choice is surgical laparoscopy, for conservative treatment, the preferred method is modified combined cystectomy. Cystectomy can be destructive for the ovary, whereas ablation may be incomplete, with a greater risk of recurrence. To the best of our knowledge, the modified combined technique seems to be more efficient in the treatment of endometriomas.
Keywords: Endometrioma; combined technique; cystectomy; laparoscopy.
Figures



Similar articles
-
A randomized controlled trial of a new technique for laparoscopic management of ovarian endometriosis preventing recurrence and keeping ovarian reserve.J Ovarian Res. 2019 Jul 20;12(1):66. doi: 10.1186/s13048-019-0542-0. J Ovarian Res. 2019. PMID: 31325962 Free PMC article. Clinical Trial.
-
Comparison between the stripping technique and the combined excisional/ablative technique for the treatment of bilateral ovarian endometriomas: a multicentre RCT.Hum Reprod. 2016 Feb;31(2):339-44. doi: 10.1093/humrep/dev313. Epub 2015 Dec 18. Hum Reprod. 2016. PMID: 26682578 Clinical Trial.
-
The impact of endometrioma and laparoscopic cystectomy on ovarian reserve and the exploration of related factors assessed by serum anti-Mullerian hormone: a prospective cohort study.J Ovarian Res. 2014 Nov 26;7:108. doi: 10.1186/s13048-014-0108-0. J Ovarian Res. 2014. PMID: 25424986 Free PMC article.
-
An update on the diagnosis, surgical management, and fertility outcomes for women with endometrioma.Acta Obstet Gynecol Scand. 2017 Jun;96(6):633-643. doi: 10.1111/aogs.13114. Epub 2017 Mar 11. Acta Obstet Gynecol Scand. 2017. PMID: 28186620 Review.
-
Risks of conservative management in women with ovarian endometriomas undergoing IVF.Hum Reprod Update. 2015 Jul-Aug;21(4):486-99. doi: 10.1093/humupd/dmv012. Epub 2015 Mar 6. Hum Reprod Update. 2015. PMID: 25750209 Review.
Cited by
-
Clinical characteristics and surgical management of endometriosis-associated infertility: A multicenter prospective cohort study.Int J Gynaecol Obstet. 2022 Oct;159(1):86-96. doi: 10.1002/ijgo.14115. Epub 2022 Feb 18. Int J Gynaecol Obstet. 2022. PMID: 35075631 Free PMC article.
-
Safety and Clinical Outcomes of Two-Session Catheter-Directed Sclerotherapy Using Ethanol for Endometrioma.Cardiovasc Intervent Radiol. 2024 Jul;47(7):901-909. doi: 10.1007/s00270-024-03700-5. Epub 2024 Mar 25. Cardiovasc Intervent Radiol. 2024. PMID: 38528174
-
Surgical Technique and Fertility Outcomes: A Comprehensive Review of Open and Laparoscopic Cystectomy in Women of Reproductive Age.Cureus. 2024 Oct 10;16(10):e71179. doi: 10.7759/cureus.71179. eCollection 2024 Oct. Cureus. 2024. PMID: 39525144 Free PMC article. Review.
-
A randomized controlled trial of a new technique for laparoscopic management of ovarian endometriosis preventing recurrence and keeping ovarian reserve.J Ovarian Res. 2019 Jul 20;12(1):66. doi: 10.1186/s13048-019-0542-0. J Ovarian Res. 2019. PMID: 31325962 Free PMC article. Clinical Trial.
-
Exploring the innovative application of cerium oxide nanoparticles for addressing oxidative stress in ovarian tissue regeneration.J Ovarian Res. 2024 Dec 5;17(1):241. doi: 10.1186/s13048-024-01566-2. J Ovarian Res. 2024. PMID: 39633503 Free PMC article. Review.
References
-
- Shebl O, Ebner T, Sommergruber M, Sir A, Tews G. Anti-Muellerian hormone serum levels in women with endometriosis: a case-control study. Gynecol Endocrinol. 2009;25:713–716. - PubMed
-
- Adamson GD. Endometriosis classification: An update. Curr Opin Obstet Gynecol. 2011;23:213–20. - PubMed
-
- Jacob F, Meier M, Caduff R, Goldstein D, Pochechueva T, Hacker N, et al. No benefit from combining HE4 and CA125 as ovarian tumor markers in a clinical setting. Gynecol Oncol. 2011;121:487–91. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources