

Perfluorocarbon in vitreoretinal surgery and preoperative bevacizumab in diabetic tractional retinal detachment
- PMID: 25317250
- PMCID: PMC4138596
- DOI: 10.4239/wjd.v5.i5.724
Perfluorocarbon in vitreoretinal surgery and preoperative bevacizumab in diabetic tractional retinal detachment
Abstract
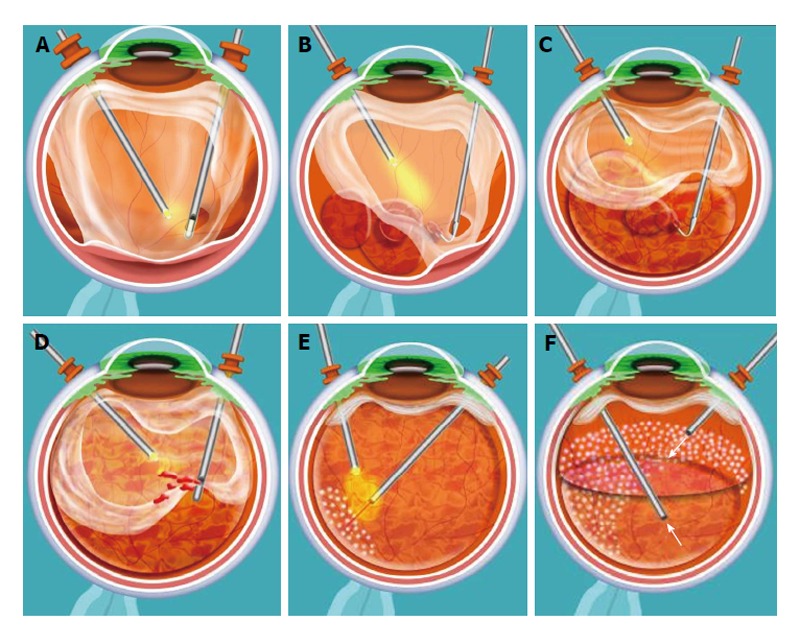
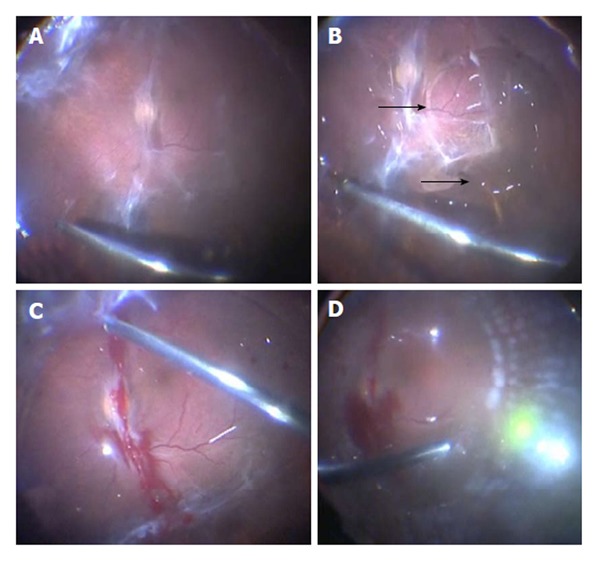
Aim: To describe the en bloc perfluorodissection (EBPD) technique and to demonstrate the applicability of using preoperative intravitreal bevacizumab during small-gauge vitreoretinal surgery (23-gauge transconjunctival sutureless vitrectomy) in eyes with advanced proliferative diabetic retinopathy (PDR) with tractional retinal detachment (TRD).
Methods: This is a prospective, interventional case series. Participants included 114 (eyes) with advanced proliferative diabetic retinopathy and TRD. EBPD was performed in 114 eyes (consecutive patients) during 23-gauge vitrectomy with the utilization of preoperative bevacizumab (1.25 mg/0.05 mL). Patients mean age was 45 years (range, 21-85 years). Surgical time had a mean of 55 min (Range, 25-85 min). Mean follow up of this group of patients was 24 mo (range, 12-32 mo). Main outcome measures included best-corrected visual acuity (BCVA), retinal reattachment, and complications.
Results: Anatomic success occurred in 100% (114/114) of eyes. Significant visual improvement [≥ 2 Early Treatment Diabetic Retinopathy Study (ETDRS) lines] was obtained in 69.2% (79/114), in 26 eyes (22.8%) BCVA remained stable, and in 8 eyes (7%) BCVA decreased (≥ 2 ETDRS lines). Final BCVA was 20/50 or better in 24% of eyes, between 20/60 and 20/400 in 46% of eyes, and worse than 20/400 in 30% of eyes. Complications included cataract in 32 (28%) eyes, iatrogenic retinal breaks in 9 (7.8%) eyes, vitreous hemorrhage requiring another procedure in 7 (6.1%) eyes, and phthisis bulbi in 1 (0.9%) eye.
Conclusion: This study demonstrates the usefulness of using preoperative intravitreal bevacizumab and EBPD during small-gauge vitreoretinal surgery in eyes with TRD in PDR.
Keywords: Avastin; Intravitreal bevacizumab; Intravitreal injections; Minimally invasive vitreoretinal surgery; Perfluorodissection; Proliferative diabetic retinopathy; Tractional retinal detachment; Vitrectomy.
Figures
References
-
- Ho T, Smiddy WE, Flynn HW. Vitrectomy in the management of diabetic eye disease. Surv Ophthalmol. 1992:190–202. - PubMed
-
- McLeod D. Microsurgical management of neovascularisation secondary to posterior segment ischaemia. Eye (Lond) 1991;5(Pt 2):252–259. - PubMed
-
- Kaiser RS, Maguire MG, Grunwald JE, Lieb D, Jani B, Brucker AJ, Maguire AM, Ho AC, Fine SL. One-year outcomes of panretinal photocoagulation in proliferative diabetic retinopathy. Am J Ophthalmol. 2000;129:178–185. - PubMed
-
- Benson WE, Brown GC, Tasman W, McNamara JA. Complications of vitrectomy for non-clearing vitreous hemorrhage in diabetic patients. Ophthalmic Surg. 1988;19:862–864. - PubMed
-
- Blankenship GW. Management of vitreous cavity hemorrhage following pars plana vitrectomy for diabetic retinopathy. Ophthalmology. 1986;93:39–44. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
