

Thrombosis as a complication of central venous access in pediatric patients with malignancies: a 5-year single-center experience
- PMID: 25317335
- PMCID: PMC4195887
- DOI: 10.1186/2052-1839-14-18
Thrombosis as a complication of central venous access in pediatric patients with malignancies: a 5-year single-center experience
Abstract
Background: Reliable central venous access (CVC) is essential for hematology-oncology patients since frequent puncture of peripheral veins-e.g., for chemotherapy, antibiotic administration, repeated blood sampling, and monitoring-can cause unacceptable pain and psychological trauma, as well as severe side effects in cases of extravasation of chemotherapy drugs. However, CVC lines still carry major risk factors, including thrombosis, infection (e.g., entry site, tunnel, and luminal infections), and catheter dislocation, leakage, or breakage.
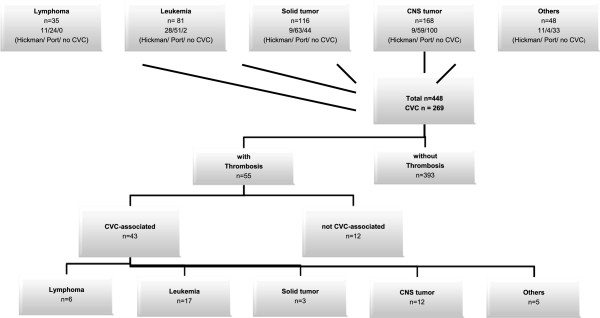
Methods: Here we performed a retrospective database analysis to determine the incidence of CVC-associated thrombosis in a single-center cohort of 448 pediatric oncologic patients, and to analyze whether any subgroup of patients was at increased risk and thus might benefit from prophylactic anticoagulation.
Results: Of the 448 patients, 269 consecutive patients received a CVC, and 55 of these 269 patients (20%) also had a thrombosis. Of these 55 patients, 43 had at least one CVC-associated thrombosis (total number of CVC-associated thrombosis: n = 52). Among all patients, the median duration of CVC exposure was 464 days. Regarding exposure time, no significant difference was found between patients with and without CVC-associated thrombosis. Subclavia catheters and advanced tumor stages seem to be the main risk factors for the development of CVC-associated thrombosis, whereas pharmacologic prophylaxis did not seem to have a relevant impact on the rate of thrombosis.
Conclusions: We conclude that pediatric surgeons and oncologists should pay close attention to ensuring optimal and accurate CVC placement, as this appears the most effective tool to minimize CVC-associated complications.
Keywords: Central venous access; Hickman catheter; Pediatric malignancy; Port; Thrombosis.
Figures


References
-
- Rouzrokh M, Shamsian BS, KhaleghNejad Tabari A, Mahmoodi M, Kouranlo J, Manafzadeh G, Arzanian MT, Fallah F, Anoush M, Abdollah Gorji F. Totally implantable subpectoral vs. subcutaneous port systems in children with malignant diseases. Arch Iran Med. 2009;12(4):389–394. - PubMed
-
- Broviac JW, Cole JJ, Scribner BH. A silicone rubber atrial catheter for prolonged parenteral alimentation. Surg Gynecol Obstet. 1973;136(4):602–606. - PubMed
-
- Niederhuber JE, Ensminger W, Gyves JW, Liepman M, Doan K, Cozzi E. Totally implanted venous and arterial access system to replace external catheters in cancer treatment. Surgery. 1982;92(4):706–712. - PubMed
-
- Nam SH, Kim DY, Kim SC, Kim IK. Complications and risk factors of infection in pediatric hemato-oncology patients with totally implantable access ports (TIAPs) Pediatr Blood Cancer. 2010;54(4):546–551. - PubMed
-
- Wiener ES, McGuire P, Stolar CJ, Rich RH, Albo VC, Ablin AR, Betcher DL, Sitarz AL, Buckley JD, Krailo MD, Versteeg C, Hammond GD. The CCSG prospective study of venous access devices: an analysis of insertions and causes for removal. J Pediatr Surg. 1992;27(2):155–163. doi: 10.1016/0022-3468(92)90304-P. - DOI - PubMed
Pre-publication history
-
- The pre-publication history for this paper can be accessed here:http://www.biomedcentral.com/2052-1839/14/18/prepub
LinkOut - more resources
Full Text Sources
Other Literature Sources
