

doi: 10.1212/CPJ.0000000000000086.
Cryptogenic stroke: A diagnostic challenge
Affiliations
- PMID: 25317376
- PMCID: PMC4196459
- DOI: 10.1212/CPJ.0000000000000086
Item in Clipboard
Cryptogenic stroke: A diagnostic challenge
Neurol Clin Pract.
2014 Oct.
Abstract
Cryptogenic, or unexplained, stroke is present in about 30%-40% of ischemic stroke patients. Pursuing a stroke mechanism is important in such patients to better choose therapy to reduce the stroke recurrence risk. Intracranial vessel imaging and cardiac evaluation with transesophageal echocardiogram and outpatient cardiac monitoring may help identify the stroke mechanism. This article highlights the diagnostic yield of various tests in identifying a stroke mechanism in stroke patients whose initial diagnostic evaluation is negative, and the implications for treatment.
Figures
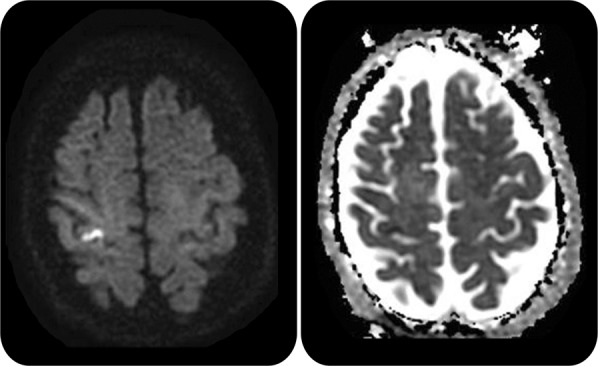
Diffusion-weighted imaging (b1000) (left) shows a hyperintense lesion along the right motor cortex (hand knob) that is hypointense on apparent diffusion coefficient map sequence (right) consistent with an acute infarct.
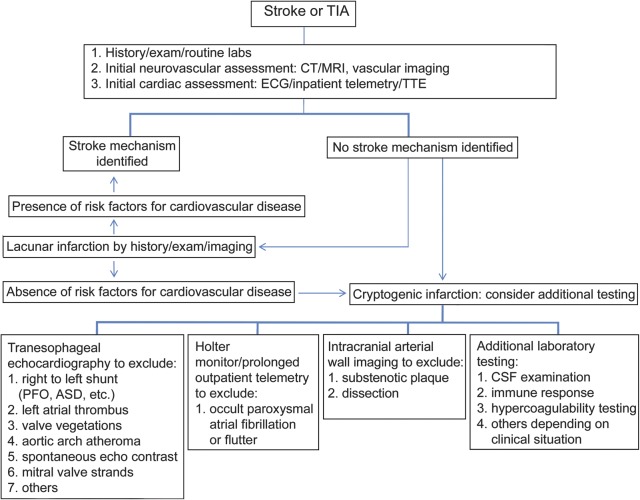
ASD = atrial septal defect; PFO = patent foramen ovale; TTE = transthoracic echocardiography.
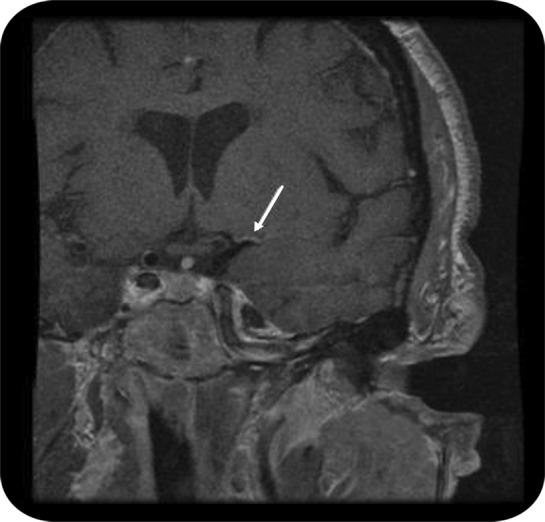
Arterial wall imaging study demonstrates enhancement consistent with atherosclerosis (arrow) in the proximal left middle cerebral artery territory in a patient with recurrent infarction in the territory of the deep white matter and basal ganglia of the left hemisphere.
References
-
- Sacco RL, Ellenberg JH, Mohr JP, et al. Infarcts of undetermined cause: the NINCDS Stroke Data Bank. Ann Neurol 1989;25:382. - PubMed
-
- Kolominsky-Rabas PL, Weber M, Gefeller O, Neundoerfer B, Heuschmann PU. Epidemiology of ischemic stroke subtypes according to TOAST criteria: incidence, recurrence, and long-term survival in ischemic stroke subtypes: a population-based study. Stroke 2001;32:2735. - PubMed
-
- Jauch EC, Saver JL, Adams HP, Jr, et al. ; American Heart Association Stroke Council; Council on Cardiovascular Nursing; Council on Peripheral Vascular Disease; Council on Clinical Cardiology. Guidelines for the early management of patients with acute ischemic stroke: a guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke 2013;44:870–947 - PubMed
-
- Adams HP, Jr, Bendixen BH, Kappelle LJ, et al. Classification of subtype of acute ischemic stroke: definitions for use in a multicenter clinical trial. TOAST: Trial of Org 10172 in Acute Stroke Treatment. Stroke 1993;24:35–41 - PubMed
-
- Ay H, Furie KL, Singhal A, Smith WS, Sorensen AG, Koroshetz WJ. An evidence-based causative classification system for acute ischemic stroke. Ann Neurol 2005;58:688–697 - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources