

Cartilage repair and subchondral bone remodeling in response to focal lesions in a mini-pig model: implications for tissue engineering
- PMID: 25318414
- PMCID: PMC4333259
- DOI: 10.1089/ten.TEA.2014.0384
Cartilage repair and subchondral bone remodeling in response to focal lesions in a mini-pig model: implications for tissue engineering
Abstract
Objective: Preclinical large animal models are essential for evaluating new tissue engineering (TE) technologies and refining surgical approaches for cartilage repair. Some preclinical animal studies, including the commonly used minipig model, have noted marked remodeling of the subchondral bone. However, the mechanisms underlying this response have not been well characterized. Thus, our objective was to compare in-vivo outcomes of chondral defects with varied injury depths and treatments.
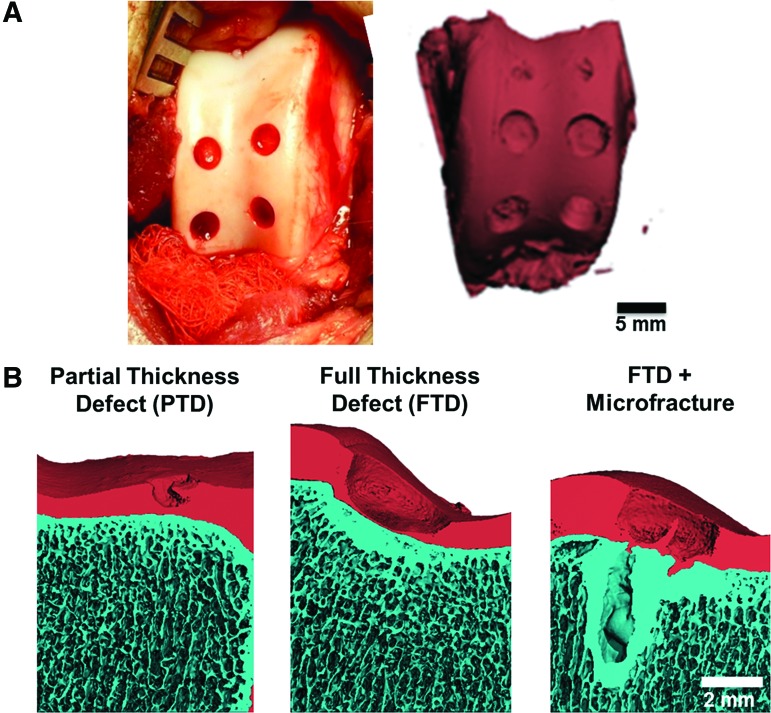
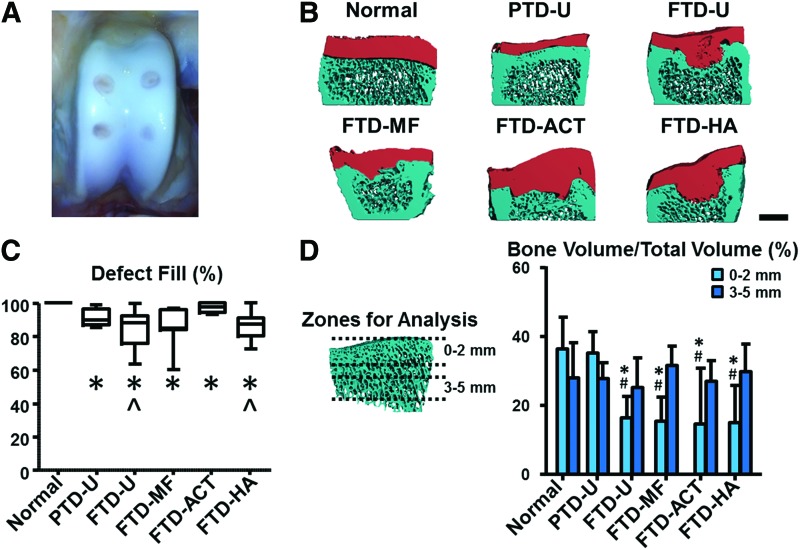
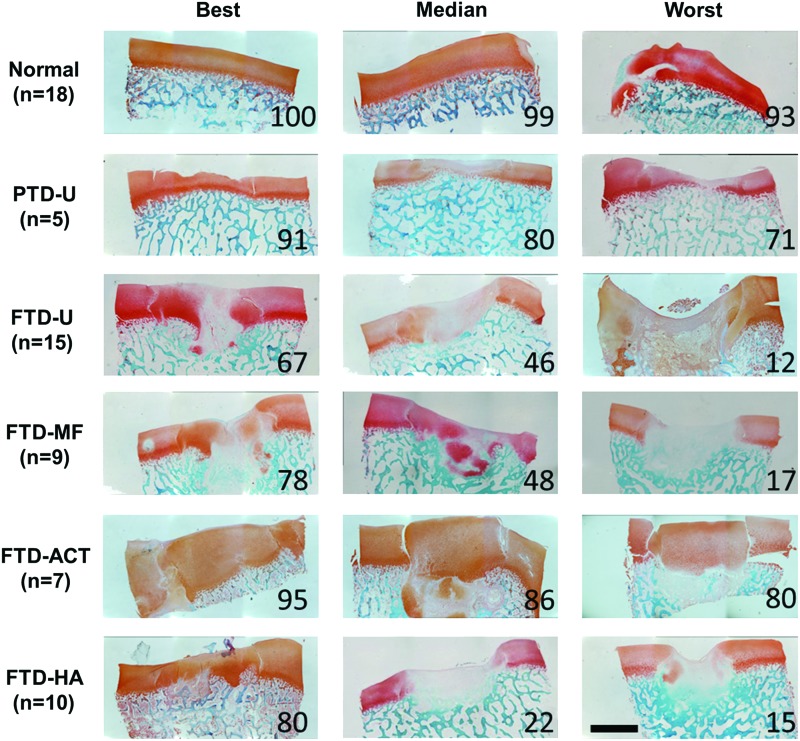
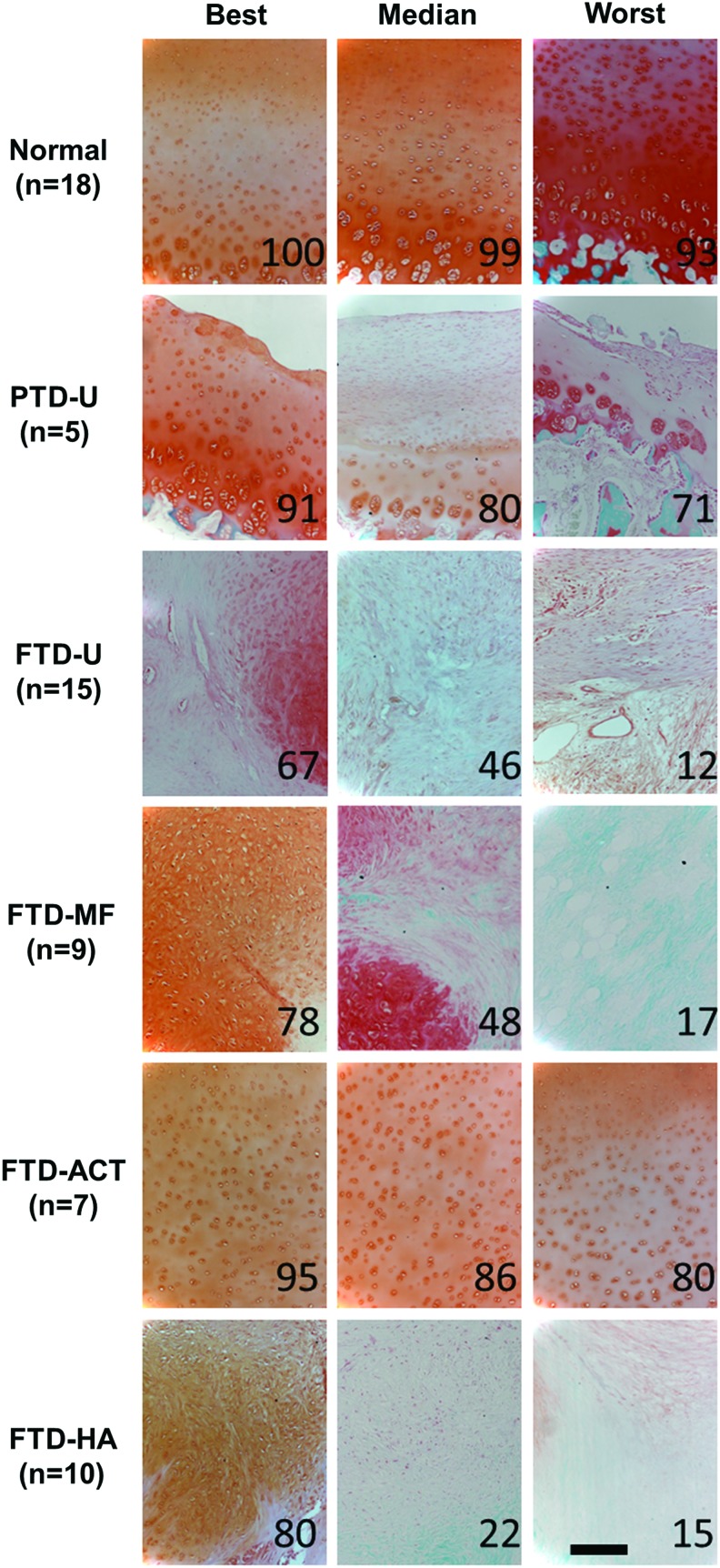
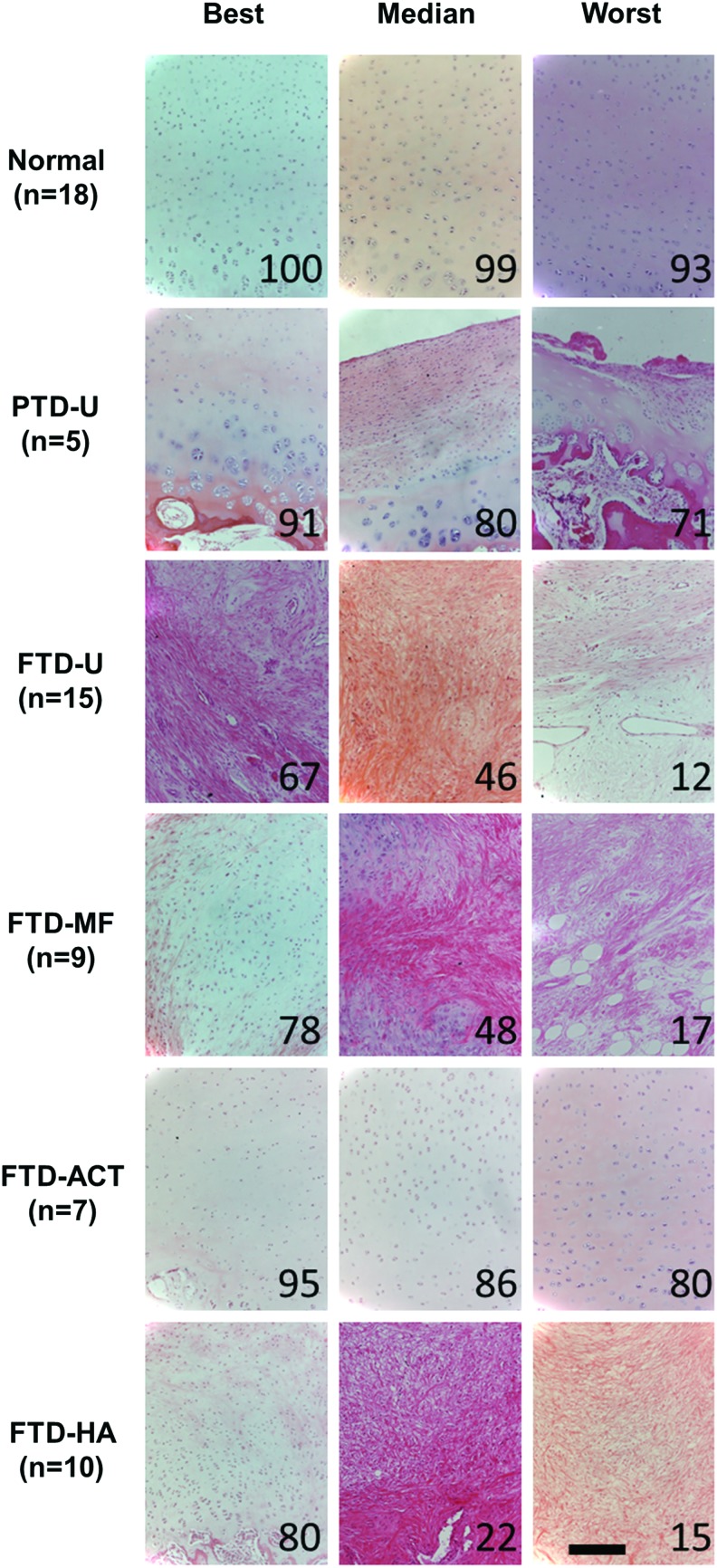
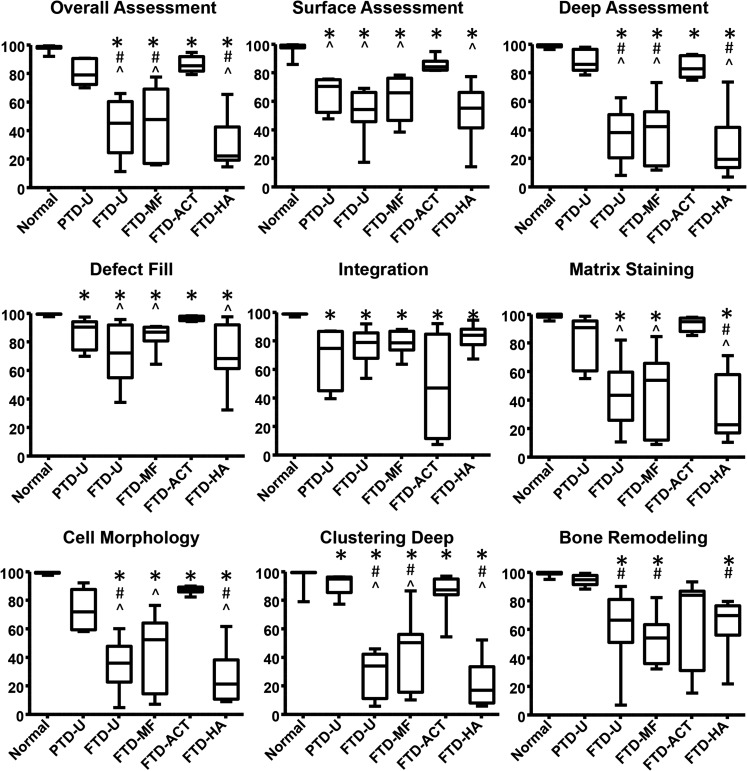
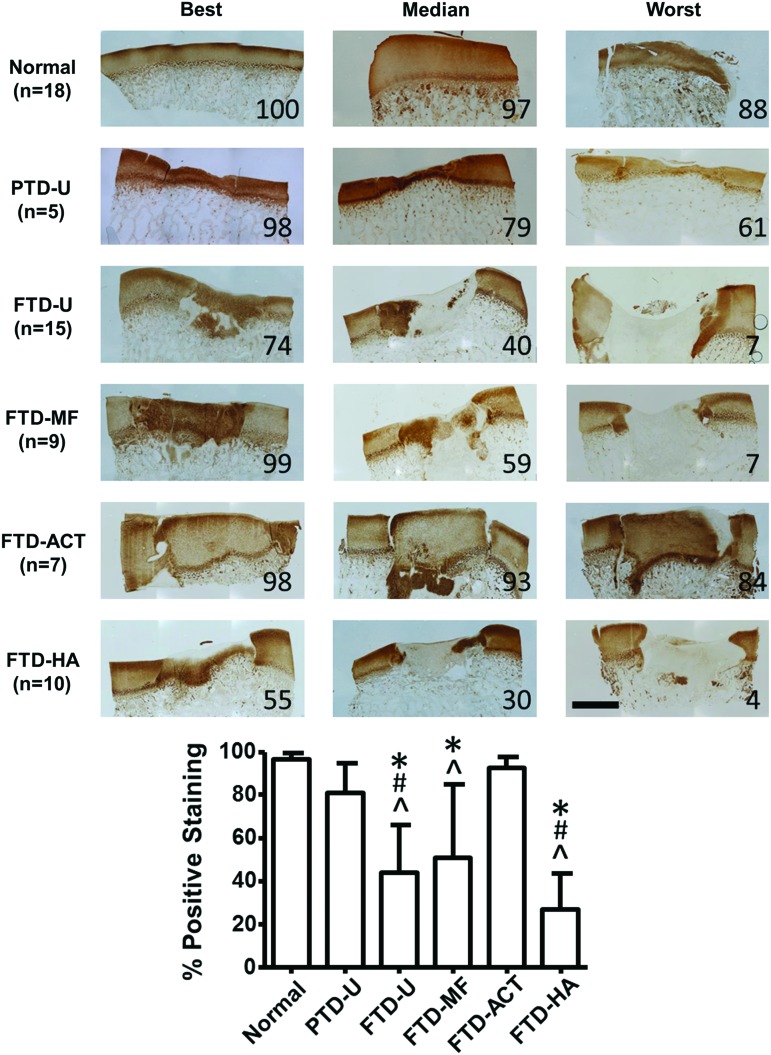
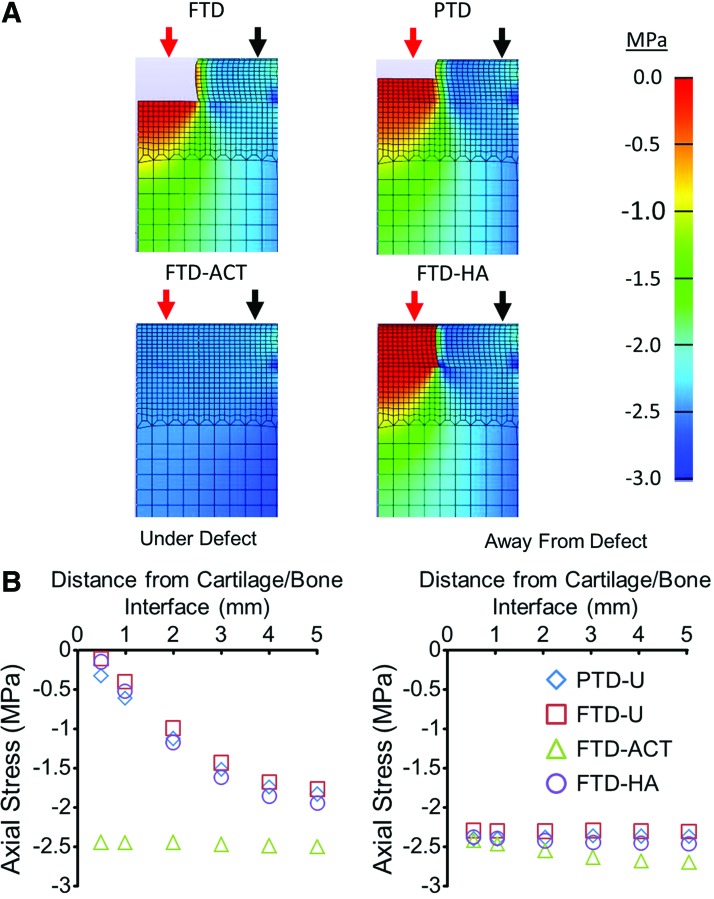
Design: Trochlear chondral defects were created in 11 Yucatan minipigs (6 months old). Groups included an untreated partial-thickness defect (PTD), an untreated full-thickness defect (FTD), and FTDs treated with microfracture, autologous cartilage transfer (FTD-ACT), or an acellular hyaluronic acid hydrogel. Six weeks after surgery, micro-computed tomography (μCT) was used to quantitatively assess defect fill and subchondral bone remodeling. The quality of cartilage repair was assessed using the ICRS-II histological scoring system and immunohistochemistry for type II collagen. A finite element model (FEM) was developed to assess load transmission.
Results: Using μCT, substantial bone remodeling was observed for all FTDs, but not for the PTD group. The best overall histological scores and greatest type II collagen staining was found for the FTD-ACT and PTD groups. The FEM confirmed that only the FTD-ACT group could initially restore appropriate transfer of compressive loads to the underlying bone.
Conclusions: The bony remodeling observed in this model system appears to be a biological phenomena and not a result of altered mechanical loading, with the depth of the focal chondral defect (partial vs. full thickness) dictating the bony remodeling response. The type of cartilage injury should be carefully controlled in studies utilizing this model to evaluate TE approaches for cartilage repair.
Figures
References
-
- Widuchowski W., Widuchowski J., and Trzaska T.Articular cartilage defects: Study of 25,124 knee arthroscopies. Knee 14,177, 2007 - PubMed
-
- Curl W.W., Krome J., Gordon E.S., Rushing J., Smith B.P., and Poehling G.G.Cartilage injuries: a review of 31,516 knee arthroscopies. Arthroscopy 13,456, 1997 - PubMed
-
- Heir S., Nerhus T.K., Rotterud J.H., Loken S., Ekeland A., Engebretsen L., and Aroen A.Focal cartilage defects in the knee impair quality of life as much as severe osteoarthritis: a comparison of knee injury and osteoarthritis outcome score in 4 patient categories scheduled for knee surgery. Am J Sports Med 38,231, 2010 - PubMed
-
- Guettler J.H., Demetropoulos C.K., Yang K.H., and Jurist K.A.Osteochondral defects in the human knee: influence of defect size on cartilage rim stress and load redistribution to surrounding cartilage. Am J Sports Med 32,1451, 2004 - PubMed
-
- Wang Y., Ding C., Wluka A.E., Davis S., Ebeling P.R., Jones G., and Cicuttini F.M.Factors affecting progression of knee cartilage defects in normal subjects over 2 years. Rheumatology (Oxford) 45,79, 2006 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
