

Pleomorphic Xanthoastrocytoma: Natural History and Long-Term Follow-Up
- PMID: 25318587
- PMCID: PMC4400218
- DOI: 10.1111/bpa.12217
Pleomorphic Xanthoastrocytoma: Natural History and Long-Term Follow-Up
Abstract
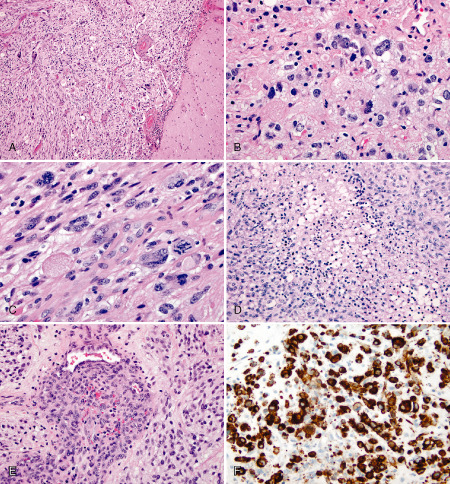
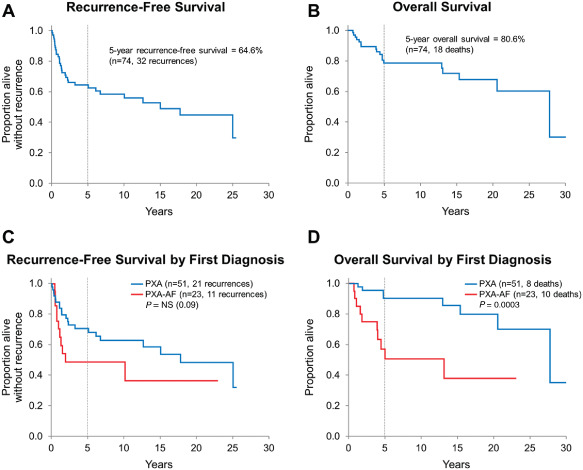
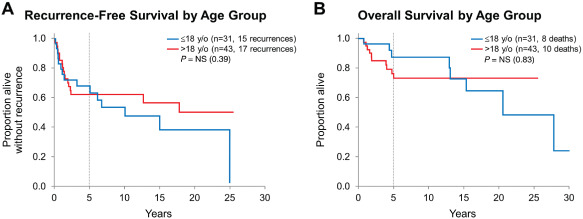
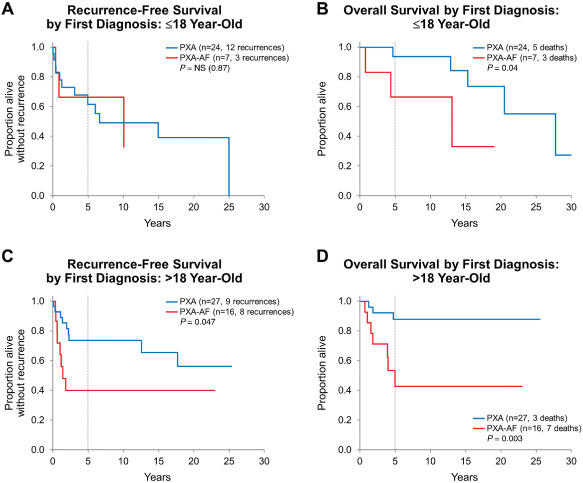
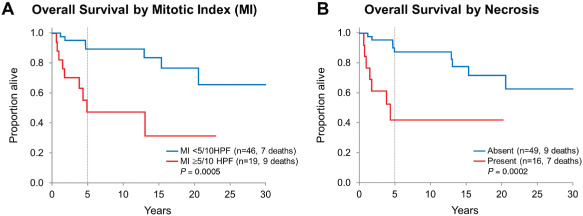
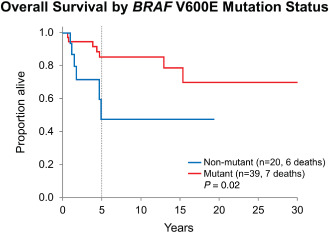
Prognostic significance of histological anaplasia and BRAF V600E mutation were retrospectively evaluated in 74 patients with pleomorphic xanthoastrocytoma (PXA). Median age at diagnosis was 21.5 years (31 pediatric, 43 adult) and median follow-up 7.6 years. Anaplasia (PXA-AF), defined as mitotic index ≥ 5/10 HPF and/or presence of necrosis, was present in 33 cases. BRAF V600E mutation was detected in 39 (of 60) cases by immunohistochemical and/or molecular analysis, all negative for IDH1 (R132H). Mitotic index ≥ 5/10 HPF and necrosis were associated with decreased overall survival (OS; P = 0.0005 and P = 0.0002, respectively). In all cases except two, necrosis was associated with mitotic index ≥ 5/10 HPF. Patients with BRAF V600E mutant tumors had significantly longer OS compared with those without BRAF V600E mutation (P = 0.02). PXA-AF patients, regardless of age, had significantly shorter OS compared with those without (P = 0.0003). Recurrence-free survival was significantly shorter for adult PXA-AF patients (P = 0.047) only. Patients who either recurred or died ≤ 3 years from diagnosis were more likely to have had either PXA-AF at first diagnosis (P = 0.008) or undergone a non-gross total resection procedure (P = 0.004) as compared with patients who did not. This study provides further evidence that PXA-AF behaves more aggressively than PXA and may qualify for WHO grade III "anaplastic" designation.
Keywords: BRAF V600E; IDH1 R132H; WHO grade; anaplastic; glioma; pleomorphic xanthoastrocytoma.
© 2014 International Society of Neuropathology.
Figures
References
-
- Alexiou GA, Moschovi M, Stefanaki K, Prodromou C, Sfakianos G, Prodromou N (2010) Malignant progression of a pleomorphic xanthoastrocytoma in a child. Neuropediatrics 41:69–71. - PubMed
-
- Arita K, Kurisu K, Tominaga A, Sugiyama K, Sumida M, Hirose T (2002) Intrasellar pleomorphic xanthoastrocytoma: case report. Neurosurgery 51:1079–1082. discussion 82. - PubMed
-
- Bagriacik EU, Baykaner MK, Yaman M, Sivrikaya G, Durdag E, Emmez H et al (2012) Establishment of a primary pleomorphic xanthoastrocytoma cell line: in vitro responsiveness to some chemotherapeutics. Neurosurgery 70:188–197. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Research Materials
Miscellaneous
