

Clinical outcomes and costs associated with in-hospital biliary complications after liver transplantation: a cross-sectional analysis
- PMID: 25319035
- PMCID: PMC4305464
- DOI: 10.1007/s11605-014-2675-1
Clinical outcomes and costs associated with in-hospital biliary complications after liver transplantation: a cross-sectional analysis
Abstract
Introduction: In-hospital biliary complications (BCs) after liver transplantation (LT) are reported in up to 20 % of patients and contribute to poor outcomes and increased costs. Existing single-center outcome and cost analyses studies are limited in scope.
Methods: This is a cross-sectional analysis of national data involving 7,967 patients transplanted between 2011 and 2012 with the primary aim of determining the association between BCs and clinical outcomes and costs. Age, race, diagnosis, and severity of illness are associated with the development of BCs.
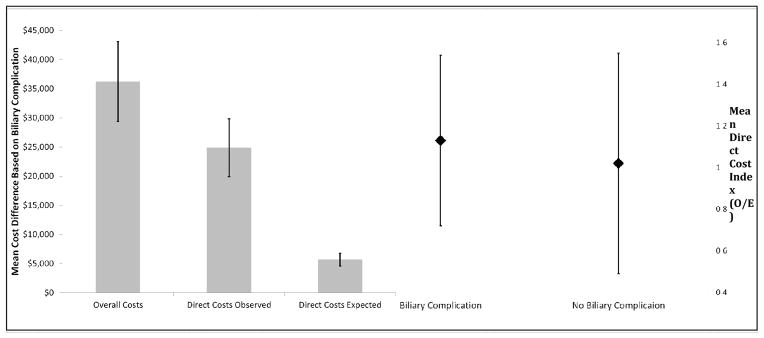
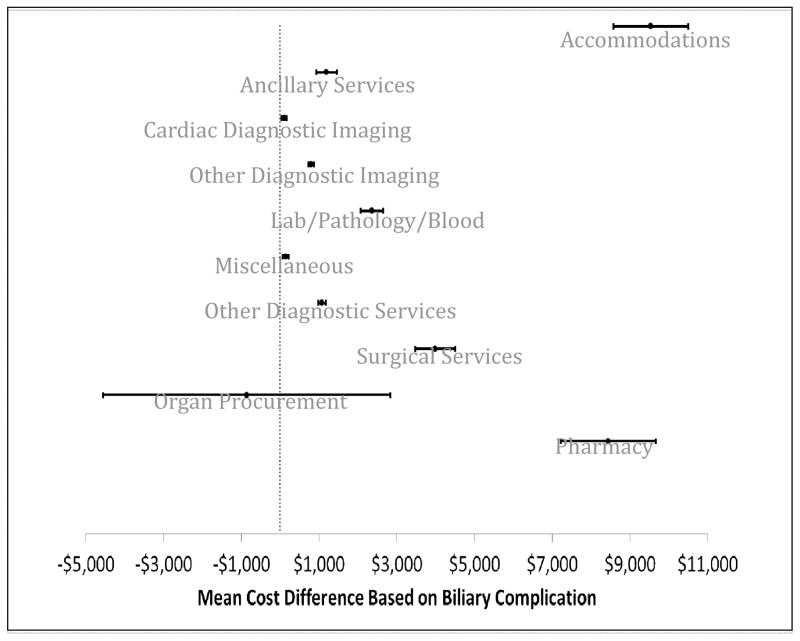
Results: BCs develop in 14.6 % of LT recipients and have substantial implications for perioperative outcomes, including length of hospital and ICU stay (27.9 vs 19.6 mean days, p < 0.001 and 12.0 vs 8.3 mean days, p < 0.001, respectively), in-hospital morbidity (39 vs 27 %, p < 0.001), 30-day readmissions (14.8 vs 11.2 %, p < 0.001), and in-hospital mortality (5.8 vs 4.0 %, p < 0.001). BCs contributed to a mean increase in in-hospital costs of $36,212 (p < 0.001), due to increases in accommodations ($9,539, p < 0.001), surgical services ($3,988, p < 0.001), and pharmacy services ($8,445, p < 0.001).
Discussion: BCs are a predominant etiology for in-hospital morbidity and mortality, while contributing significantly to the high cost of LT. Efforts should be focused on understanding salient and modifiable risk factors, while developing innovative strategies to reduce BCs.
Conflict of interest statement
No authors have any competing interests. An ethics statement was not required for this work.
Figures
References
-
- Heidenhain C, Heise M, Jonas S, Ben-Asseur M, Puhl G, Mittler J, et al. Retrograde reperfusion via vena cava lowers the risk of initial nonfunction but increases the risk of ischemic-type biliary lesions in liver transplantation--a randomized clinical trial. Transpl Int. 2006;19(9):738–48. - PubMed
-
- Sanchez-Urdazpal L, Gores GJ, Ward EM, Maus TP, Wahlstrom HE, Moore SB, et al. Ischemic-type biliary complications after orthotopic liver transplantation. Hepatology. 1992;16(1):49–53. - PubMed
-
- Adam R, Bismuth H, Diamond T, Ducot B, Morino M, Astarcioglu I, et al. Effect of extended cold ischaemia with UW solution on graft function after liver transplantation. Lancet. 1992;340(8832):1373–6. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
