

Retrograde stapling of a free cervical jejunal interposition graft: a technical innovation and case report
- PMID: 25319372
- PMCID: PMC4202252
- DOI: 10.1186/1471-2482-14-78
Retrograde stapling of a free cervical jejunal interposition graft: a technical innovation and case report
Abstract
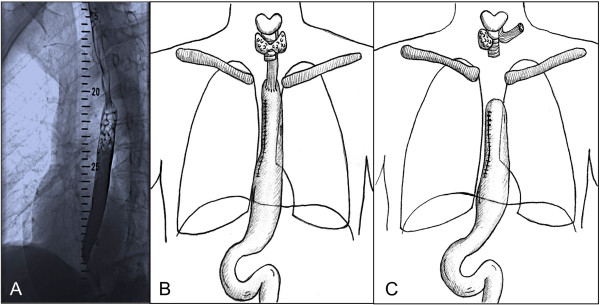
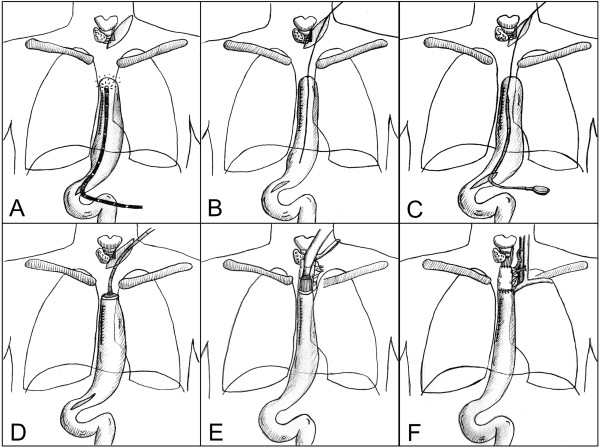
Background: Free jejunal interposition is a useful technique for reconstruction of the cervical esophagus. However, the distal anastomosis between the graft and the remaining thoracic esophagus or a gastric conduit can be technically challenging when located very low in the thoracic aperture. We here describe a modified technique for retrograde stapling of a jejunal graft to a failed gastric conduit using a circular stapler on a delivery system.
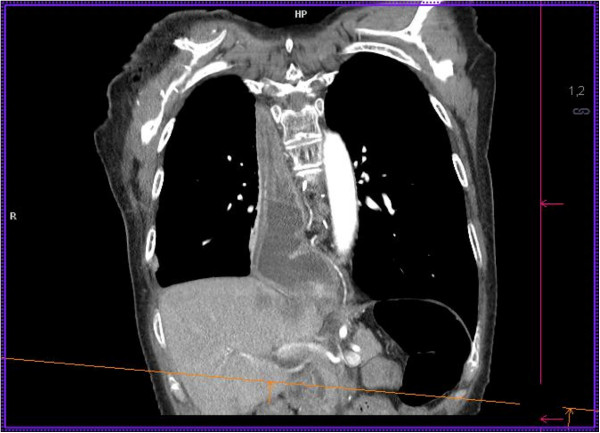
Case presentation: A 56 year-old patient had been referred for esophageal squamous cell carcinoma at 20 cm from the incisors. On day 8 after thoracoabdominal esophagectomy with gastric pull-up, an anastomotic leakage was diagnosed. A proximal-release stent was successfully placed by gastroscopy and the patient was discharged. Two weeks later, an esophagotracheal fistula occurred proximal to the esophageal stent. Cervical esophagostomy was performed with cranial closure of the gastric conduit, which was left in situ within the right hemithorax. Three months later, reconstruction was performed using a free jejunal interposition. The anvil of a circular stapler (Orvil®, Covidien) was placed transabdominally through an endoscopic rendez-vous procedure into the gastric conduit. A free jejunal graft was retrogradely stapled to the proximal end of the conduit. Microvascular anastomoses were performed subsequently. The proximal anastomosis of the conduit was completed manually after reperfusion.
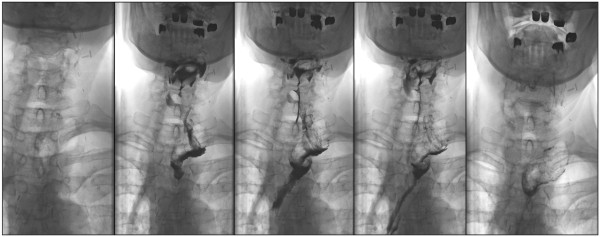
Conclusions: This modified technique allows stapling of a jejunal interposition graft located deep in the thoracic aperture and is therefore a useful method that may help to avoid reconstruction by colonic pull-up and thoracotomy.
Figures
Similar articles
-
A safe and reproducible anastomotic technique for minimally invasive Ivor Lewis oesophagectomy: the circular-stapled anastomosis with the trans-oral anvil.Eur J Cardiothorac Surg. 2010 Jun;37(6):1421-6. doi: 10.1016/j.ejcts.2010.01.010. Epub 2010 Feb 12. Eur J Cardiothorac Surg. 2010. PMID: 20153660 Free PMC article.
-
Thoracoscopic Esophagojejunostomy in the Upper Mediastinum After Thoracoscopic Esophagectomy with Total Gastrectomy.J Laparoendosc Adv Surg Tech A. 2016 Sep;26(9):715-20. doi: 10.1089/lap.2016.0056. Epub 2016 Apr 19. J Laparoendosc Adv Surg Tech A. 2016. PMID: 27093095
-
Fallback technique with circular stapler prevents anastomotic obstruction after esophagectomy: A case report of surgical approach.Medicine (Baltimore). 2019 Feb;98(8):e13571. doi: 10.1097/MD.0000000000013571. Medicine (Baltimore). 2019. PMID: 30813121 Free PMC article.
-
Restoring the perfusion of accidentally transected right gastroepiploic vessels during gastric conduit harvest for esophagectomy using microvascular anastomosis: a case report and literature review.BMC Surg. 2022 Jul 28;22(1):292. doi: 10.1186/s12893-022-01728-3. BMC Surg. 2022. PMID: 35902899 Free PMC article. Review.
-
Gastric conduit reconstruction after esophagectomy.Dis Esophagus. 2024 Oct 2;37(10):doae045. doi: 10.1093/dote/doae045. Dis Esophagus. 2024. PMID: 38762331 Review.
Cited by
-
Ileo-right hemi-colonic cervical pull-up on a non-supercharged ileocolic arterial pedicle: A technical and case report.World J Gastroenterol. 2016 Apr 14;22(14):3869-74. doi: 10.3748/wjg.v22.i14.3869. World J Gastroenterol. 2016. PMID: 27076773 Free PMC article.
References
-
- Clavien PA, Sarr MG, Fong YE. Atlas of Upper Gastrointestinal and Hepato-Pancreato-Biliary Surgery. Springer. 2007;XXVIII:48ff.
-
- Carrel A. The surgery of blood vessels. Johns Hopkins Hosp Bull. 1907;190:18–28.
-
- Roux C. A new operation for intractable obstruction of the esophagus (L'oesophagp-jejunogastrosiose, nouvelle operation pour retreciccement infrachissable del'oesophagus) Semin Med. 1907;27:34–40.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
