

Diffusion abnormalities on intraoperative magnetic resonance imaging as an early predictor for the risk of posterior fossa syndrome
- PMID: 25319997
- PMCID: PMC4483076
- DOI: 10.1093/neuonc/nou299
Diffusion abnormalities on intraoperative magnetic resonance imaging as an early predictor for the risk of posterior fossa syndrome
Abstract
Background: Posterior fossa syndrome (PFS) is an important complication of posterior fossa surgery in children. The pathophysiology of this condition remains unclear, but there is evidence implicating surgical injury of the proximal efferent cerebellar pathway (pECP) and the cerebellar vermis to PFS. We aimed to evaluate if diffusion abnormalities involving these structures on the final intraoperative MRI can predict the development of PFS.
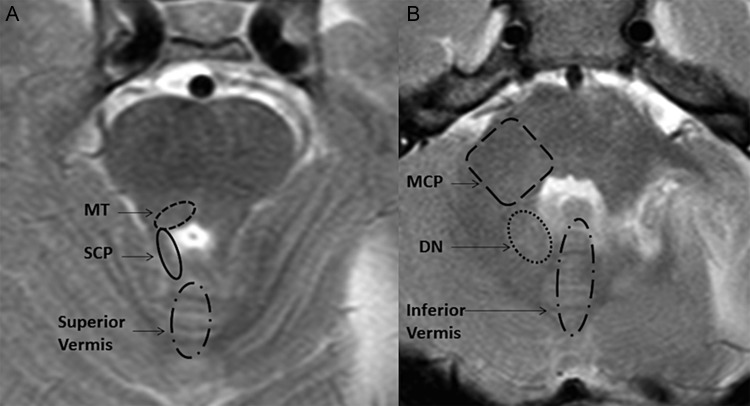
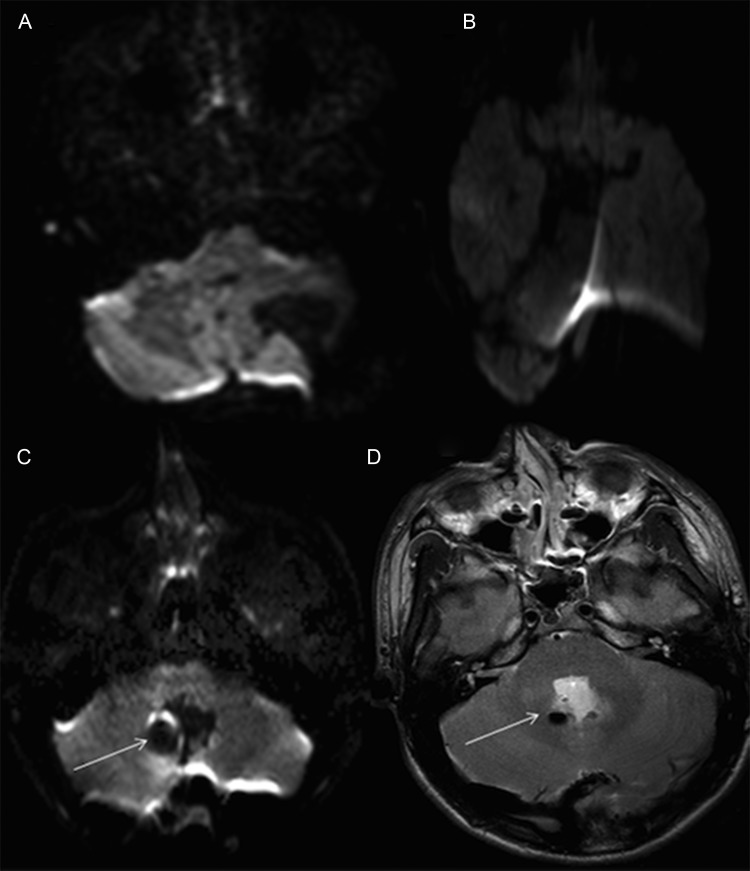
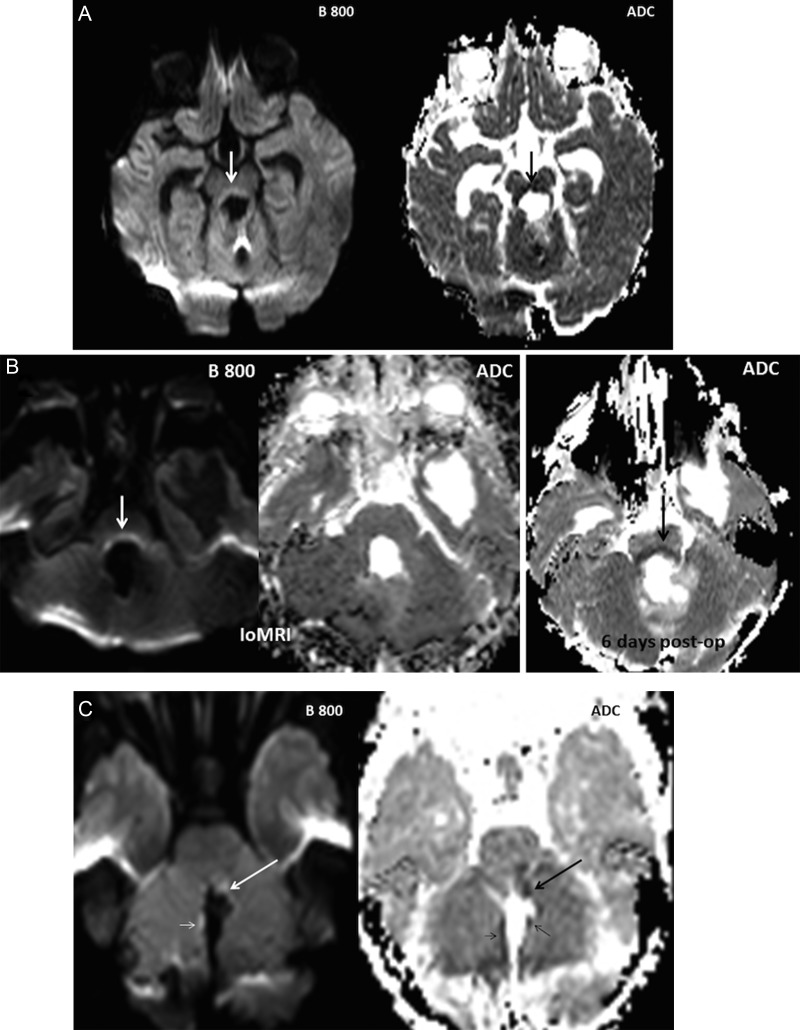
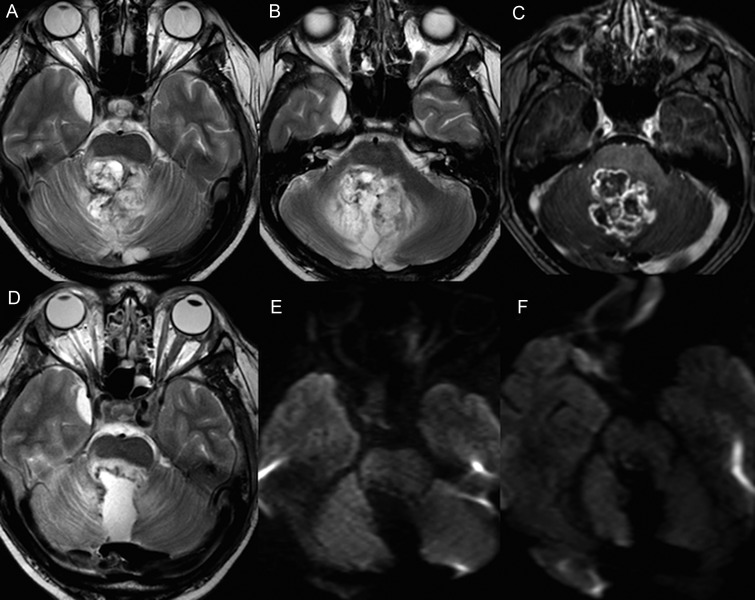
Methods: Diffusion-weighted imaging from 31 posterior fossa resections were anonymized and evaluated for abnormalities involving the dentate nucleus, superior cerebellar peduncle, and the mesencephalic tegmentum forming the pECP, vermis, and middle cerebellar peduncle. The case notes were independently evaluated for evidence of PFS.
Results: The diffusion imaging in 28 cases was of optimal quality for evaluation. Diffusion abnormalities were identified in 10 cases, 7 of which involved the pECP. Retrospective evaluation revealed evidence of PFS in 6 cases. There was a significant association between abnormalities involving pECP structures (P = .001) and development of PFS. Bilateral involvement of pECP (P = .006) was a highly specific risk factor for predicting the development of PFS. Diffusion abnormality of the inferior vermis was significantly associated with PFS (P = .001) but may not represent a risk factor in isolation.
Conclusion: This study demonstrates the feasibility of identifying children at risk for developing PFS at the earliest stage post tumor resection and thus adds to the growing evidence base on its pathophysiology.
Keywords: cerebellar mutism syndrome; diffusion-weighted imaging; efferent cerebellar pathway; intraoperative MRI; posterior fossa syndrome.
© The Author(s) 2014. Published by Oxford University Press on behalf of the Society for Neuro-Oncology. All rights reserved. For permissions, please e-mail: journals.permissions@oup.com.
Figures
References
-
- Rekate HL, Grubb RL, Aram DM, et al. Muteness of cerebellar origin. Arch Neurol. 1985;42(7):697–698. - PubMed
-
- Pollack IF, Polinko P, Albright AL, et al. Mutism and pseudobulbar symptoms after resection of posterior fossa tumors in children: incidence and pathophysiology. Neurosurgery. 1995;37(5):885–893. - PubMed
-
- Gudrunardottir T, Sehested A, Juhler M, et al. Cerebellar mutism: review of the literature. Childs Nerv Syst. 2011;27(3):355–363. - PubMed
-
- Steinbok P, Cochrane DD, Perrin R, et al. Mutism after posterior fossa tumour resection in children: incomplete recovery on long-term follow-up. Pediatr Neurosurg. 2003;39(4):179–183. - PubMed
-
- Huber JF, Bradley K, Spiegler BJ, et al. Long-term effects of transient cerebellar mutism after cerebellar astrocytoma or medulloblastoma tumor resection in childhood. Childs Nerv Syst. 2006;22(2):132–138. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
