

Management and clinical outcomes in patients treated with apixaban vs warfarin undergoing procedures
- PMID: 25320240
- PMCID: PMC4263979
- DOI: 10.1182/blood-2014-08-595496
Management and clinical outcomes in patients treated with apixaban vs warfarin undergoing procedures
Abstract
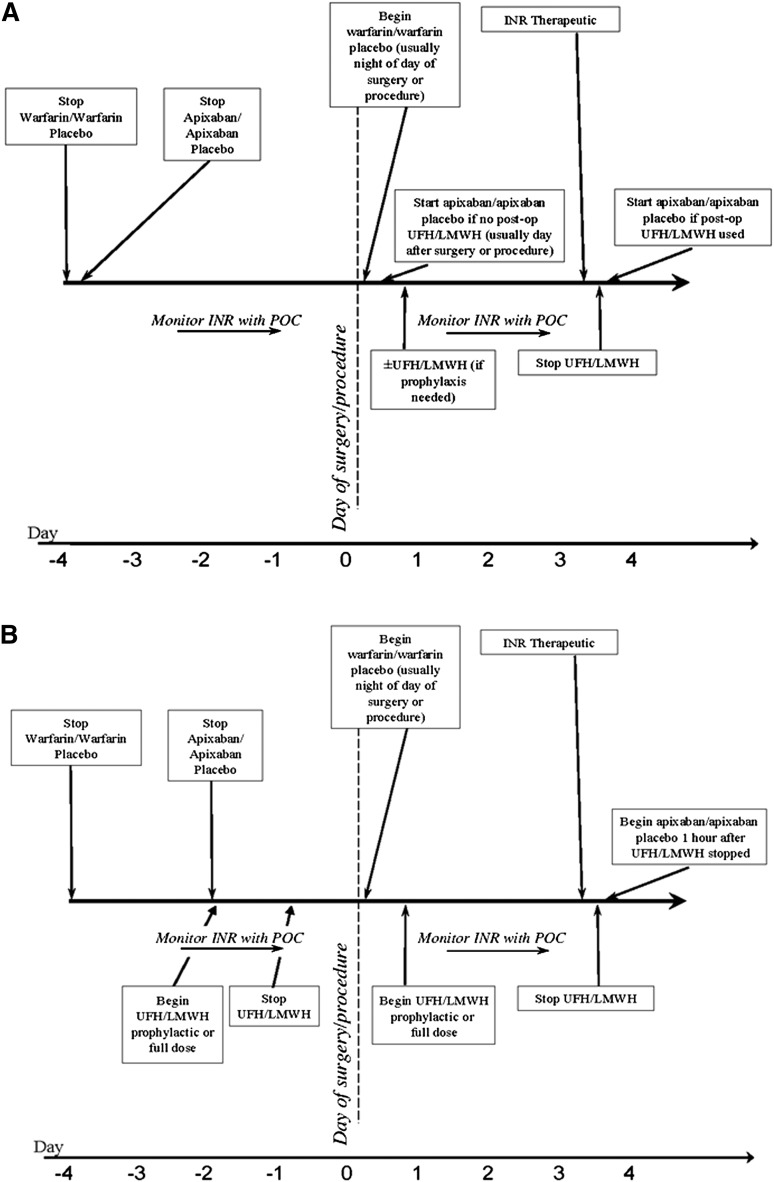
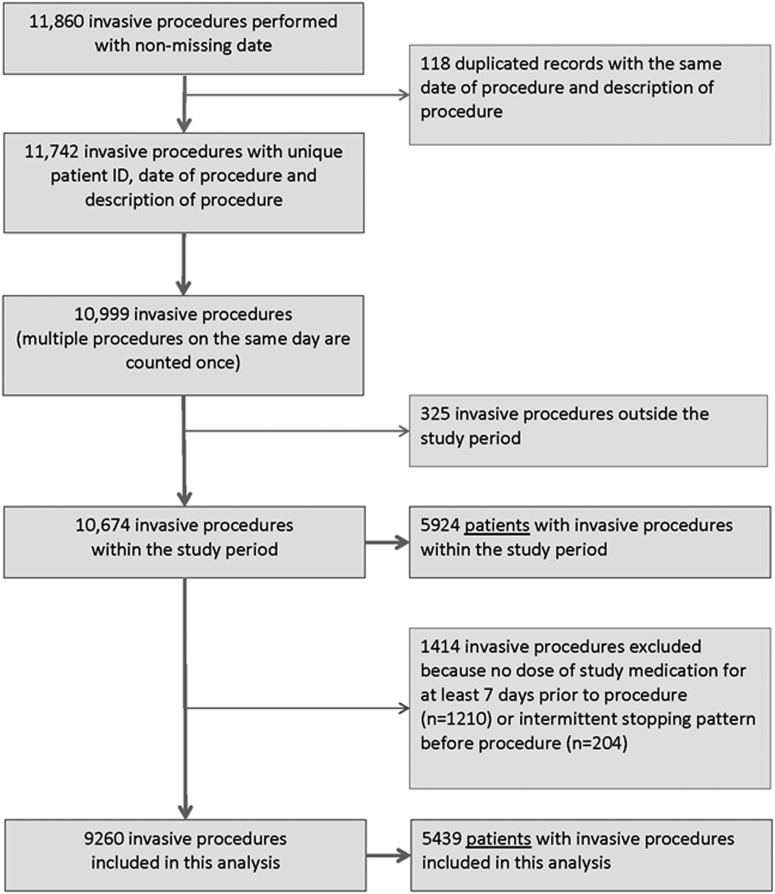
Using data from ARISTOTLE, we describe the periprocedural management of anticoagulation and rates of subsequent clinical outcomes among patients chronically anticoagulated with warfarin or apixaban. We recorded whether (and for how long) anticoagulant therapy was interrupted preprocedure, whether bridging therapy was used, and the proportion of patients who experienced important clinical outcomes during the 30 days postprocedure. Of 10 674 procedures performed during follow-up in 5924 patients, 9260 were included in this analysis. Anticoagulant treatment was not interrupted preprocedure 37.5% of the time. During the 30 days postprocedure, stroke or systemic embolism occurred after 16/4624 (0.35%) procedures among apixaban-treated patients and 26/4530 (0.57%) procedures among warfarin-treated patients (odds ratio [OR] 0.601; 95% confidence interval [CI] 0.322-1.120). Major bleeding occurred in 74/4560 (1.62%) procedures in the apixaban arm and 86/4454 (1.93%) in the warfarin arm (OR 0.846; 95% CI 0.614-1.166). The risk of death was similar with apixaban (54/4624 [1.17%]) and warfarin (49/4530 [1.08%]) (OR 1.082; 95% CI 0.733-1.598). Among patients in ARISTOTLE, the 30-day postprocedure stroke, death, and major bleeding rates were low and similar in apixaban- and warfarin-treated patients, regardless of whether anticoagulation was stopped beforehand. Our findings suggest that many patients on chronic anticoagulation can safely undergo procedures; some will not require a preprocedure interruption of anticoagulation. ARISTOTLE was registered at www.clinicaltrials.gov as #NCT00412984.
© 2014 by The American Society of Hematology.
Figures
References
-
- Granger CB, Alexander JH, McMurray JJ, et al. ARISTOTLE Committees and Investigators. Apixaban versus warfarin in patients with atrial fibrillation. N Engl J Med. 2011;365(11):981–992. - PubMed
-
- Garcia D, Libby E, Crowther MA. The new oral anticoagulants. Blood. 2010;115(1):15–20. - PubMed
-
- Healey JS, Eikelboom J, Douketis J, et al. RE-LY Investigators. Periprocedural bleeding and thromboembolic events with dabigatran compared with warfarin: results from the Randomized Evaluation of Long-Term Anticoagulation Therapy (RE-LY) randomized trial. Circulation. 2012;126(3):343–348. - PubMed
-
- Lopes RD, Alexander JH, Al-Khatib SM, et al. ARISTOTLE Investigators. Apixaban for reduction in stroke and other ThromboemboLic events in atrial fibrillation (ARISTOTLE) trial: design and rationale. Am Heart J. 2010;159(3):331–339. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
