

Pathology of pancreatic ductal adenocarcinoma: facts, challenges and future developments
- PMID: 25320520
- PMCID: PMC4194566
- DOI: 10.3748/wjg.v20.i38.13833
Pathology of pancreatic ductal adenocarcinoma: facts, challenges and future developments
Abstract
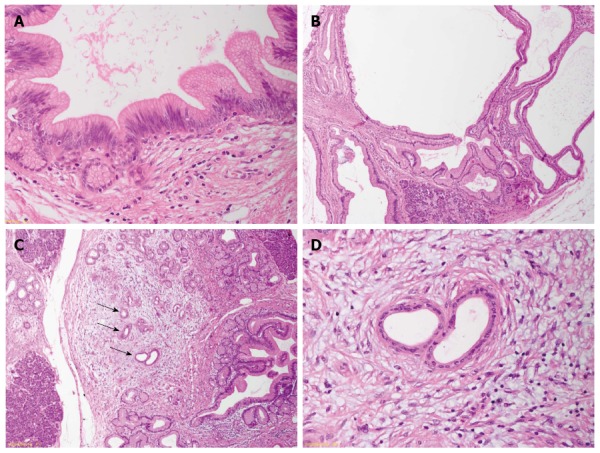
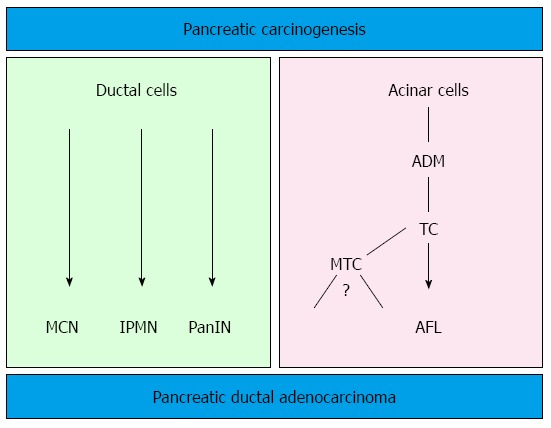
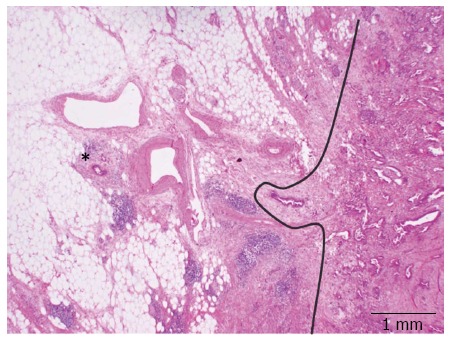
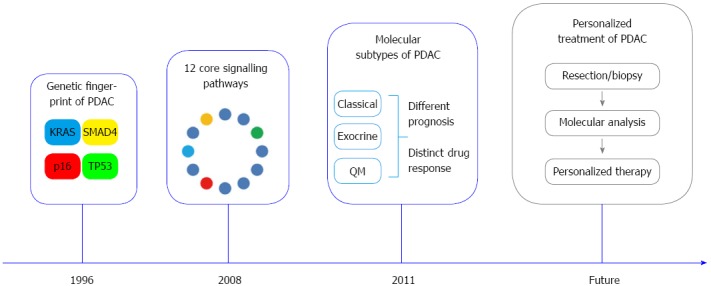
Despite major improvements concerning its diagnosis and treatment, pancreatic ductal adenocarcinoma (PDAC) remains an aggressive disease with an extremely poor prognosis. Pathology, as interface discipline between basic and clinical medicine, has substantially contributed to the recent developments and has laid the basis for further progress. The definition and classification of precursor lesions of PDAC and their molecular characterization is a fundamental step for the potential identification of biomarkers and the development of imaging methods for early detection. In addition, by integrating findings in humans with the knowledge acquired through the investigation of transgenic mouse models for PDAC, a new model for pancreatic carcinogenesis has been proposed and partially validated in individuals with genetic predisposition for PDAC. The introduction and validation of a standardized system for pathology reporting based on the axial slicing technique has shown that most pancreatic cancer resections are R1 resections and that this is due to inherent anatomical and biological properties of PDAC. This standardized assessment of prognostic relevant parameters represents the basis for the successful conduction of multicentric studies and for the interpretation of their results. Finally, recent studies have shown that distinct molecular subtypes of PDAC exist and are associated with different prognosis and therapy response. The prospective validation of these results and the integration of molecular analyses in a comprehensive pathology report in the context of individualised cancer therapy represent a major challenge for the future.
Keywords: Atypical flat lesion; Molecular subtypes; Pancreatic cancer; Pancreatic ductal adenocarcinoma; Precursor lesions; R1.
Figures
References
-
- Hidalgo M. Pancreatic cancer. N Engl J Med. 2010;362:1605–1617. - PubMed
-
- Hidalgo M. New insights into pancreatic cancer biology. Ann Oncol. 2012;23 Suppl 10:x135–x138. - PubMed
-
- Hruban RH, Adsay NV, Albores-Saavedra J, Compton C, Garrett ES, Goodman SN, Kern SE, Klimstra DS, Klöppel G, Longnecker DS, et al. Pancreatic intraepithelial neoplasia: a new nomenclature and classification system for pancreatic duct lesions. Am J Surg Pathol. 2001;25:579–586. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
