

Chemotherapy induced liver abnormalities: an imaging perspective
- PMID: 25320738
- PMCID: PMC4197183
- DOI: 10.3350/cmh.2014.20.3.317
Chemotherapy induced liver abnormalities: an imaging perspective
Abstract
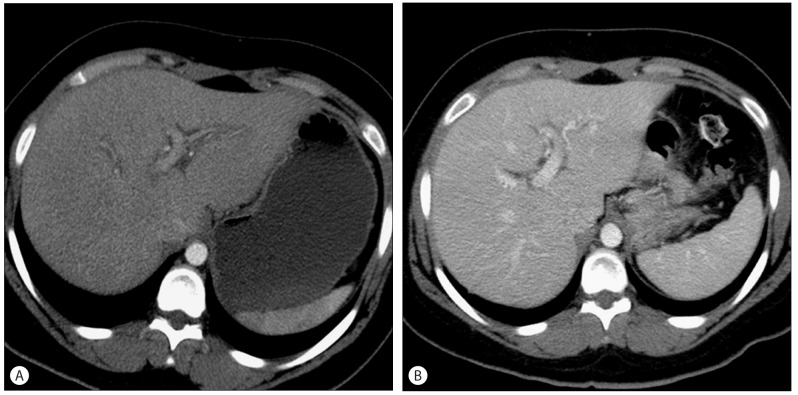
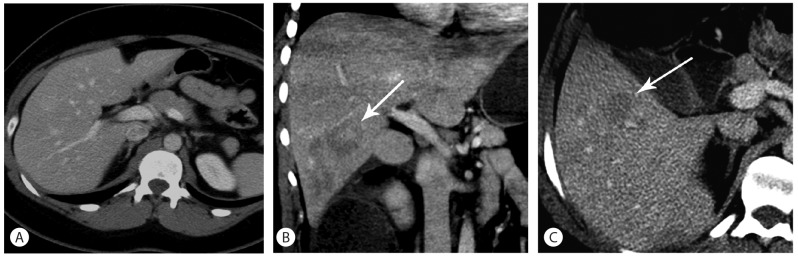
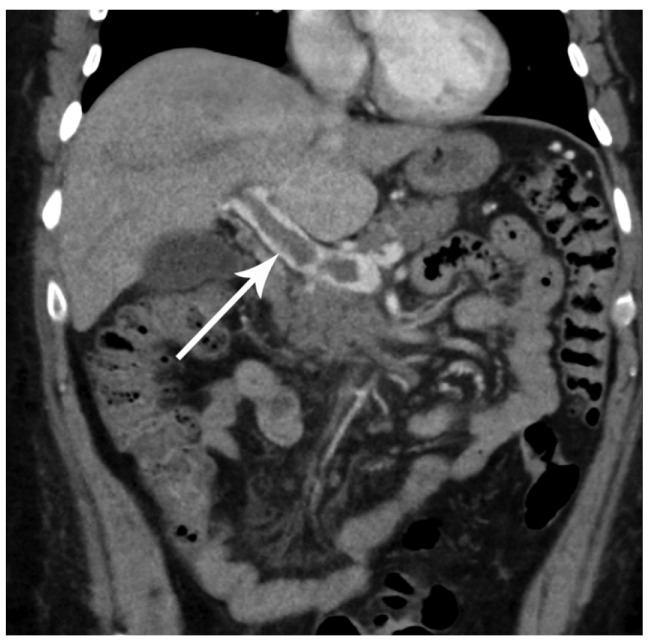
Treating patients undergoing chemotherapy who display findings of liver toxicity, requires a solid understanding of these medications. It is important for any clinician to have an index of suspicion for liver toxicity and be able to recognize it, even on imaging. Cancer chemotherapy has evolved, and newer medications that target cell biology have a different pattern of liver toxicity and may differ from the more traditional cytotoxic agents. There are several hepatic conditions that can result and keen clinical as well as radiographic recognition are paramount. Conditions such as sinusoidal obstructive syndrome, steatosis, and pseudocirrhosis are more commonly associated with chemotherapy. These conditions can display clinical signs of acute hepatitis, liver cirrhosis, and even liver failure. It is important to anticipate and recognize these adverse reactions and thus appropriate clinical action can be taken. Often times, patients with these liver manifestations can be managed with supportive therapies, and liver toxicity may resolve after discontinuation of chemotherapy.
Keywords: Chemotherapy; Hepatic Necrosis; Hepatic toxicity; Hepatitis; Pseudocirrhosis; Steatosis.
Conflict of interest statement
The authors have no conflicts to disclose.
Figures

References
-
- Torrisi JM, Schwartz LH, Gollub MJ, Ginsberg MS, Bosl GJ, Hricak H. CT findings of chemotherapy-induced toxicity: what radiologists need to know about the clinical and radiologic manifestations of chemotherapy toxicity. Radiology. 2011;258:41–56. - PubMed
-
- Bar J, Onn A. Combined anti-proliferative and anti-angiogenic strategies for cancer. Expert Opin Pharmacother. 2008;9:701–715. - PubMed
-
- King PD, Perry MC. Hepatotoxicity of chemotherapy. Oncologist. 2001;6:162–176. - PubMed
-
- Shaunak S, Munro JM, Weinbren K, Walport MJ, Cox TM. Cyclophosphamide-induced liver necrosis: a possible interaction with azathioprine. Q J Med. 1988;67:309–317. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
