

Patient-centric blood pressure-targeted cardiopulmonary resuscitation improves survival from cardiac arrest
- PMID: 25321490
- PMCID: PMC4315818
- DOI: 10.1164/rccm.201407-1343OC
Patient-centric blood pressure-targeted cardiopulmonary resuscitation improves survival from cardiac arrest
Abstract
Rationale: Although current resuscitation guidelines are rescuer focused, the opportunity exists to develop patient-centered resuscitation strategies that optimize the hemodynamic response of the individual in the hopes to improve survival.
Objectives: To determine if titrating cardiopulmonary resuscitation (CPR) to blood pressure would improve 24-hour survival compared with traditional CPR in a porcine model of asphyxia-associated ventricular fibrillation (VF).
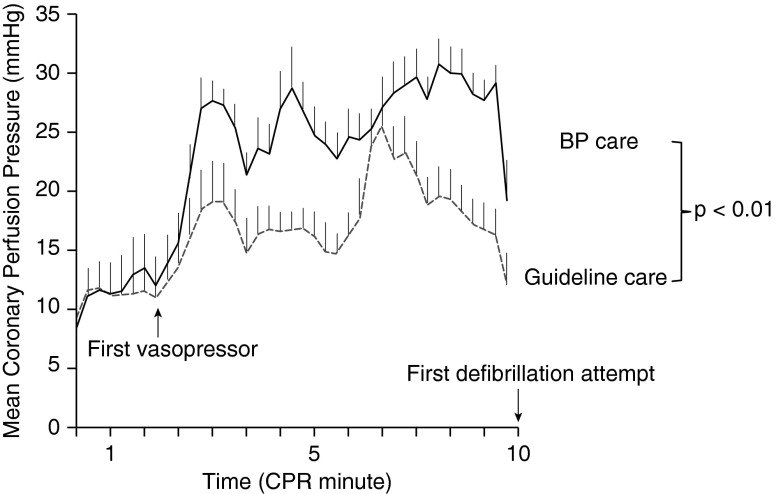
Methods: After 7 minutes of asphyxia, followed by VF, 20 female 3-month-old swine randomly received either blood pressure-targeted care consisting of titration of compression depth to a systolic blood pressure of 100 mm Hg and vasopressors to a coronary perfusion pressure greater than 20 mm Hg (BP care); or optimal American Heart Association Guideline care consisting of depth of 51 mm with standard advanced cardiac life support epinephrine dosing (Guideline care). All animals received manual CPR for 10 minutes before first shock. Primary outcome was 24-hour survival.
Measurements and main results: The 24-hour survival was higher in the BP care group (8 of 10) compared with Guideline care (0 of 10); P = 0.001. Coronary perfusion pressure was higher in the BP care group (point estimate +8.5 mm Hg; 95% confidence interval, 3.9-13.0 mm Hg; P < 0.01); however, depth was higher in Guideline care (point estimate +9.3 mm; 95% confidence interval, 6.0-12.5 mm; P < 0.01). Number of vasopressor doses before first shock was higher in the BP care group versus Guideline care (median, 3 [range, 0-3] vs. 2 [range, 2-2]; P = 0.003).
Conclusions: Blood pressure-targeted CPR improves 24-hour survival compared with optimal American Heart Association care in a porcine model of asphyxia-associated VF cardiac arrest.
Keywords: asphyxia; heart arrest; vascular access devices.
Figures

Comment in
-
Goal-directed cardiopulmonary resuscitation for patients in intensive care units.Am J Respir Crit Care Med. 2014 Dec 1;190(11):1205-6. doi: 10.1164/rccm.201411-1971ED. Am J Respir Crit Care Med. 2014. PMID: 25436778 No abstract available.
References
-
- Neumar RW, Otto CW, Link MS, Kronick SL, Shuster M, Callaway CW, Kudenchuk PJ, Ornato JP, McNally B, Silvers SM, et al. Part 8: adult advanced cardiovascular life support: 2010 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation. 2010;122(18) Suppl. 3:S729–S767. - PubMed
-
- Kleinman ME, Chameides L, Schexnayder SM, Samson RA, Hazinski MF, Atkins DL, Berg MD, de Caen AR, Fink EL, Freid EB, et al. Part 14: pediatric advanced life support: 2010 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Circulation 2010122;18Suppl. 3S876–S908. - PubMed
-
- Merchant RM, Yang L, Becker LB, Berg RA, Nadkarni V, Nichol G, Carr BG, Mitra N, Bradley SM, Abella BS, et al. American Heart Association Get With The Guidelines-Resuscitation Investigators. Incidence of treated cardiac arrest in hospitalized patients in the United States. Crit Care Med. 2011;39:2401–2406. - PMC - PubMed
-
- Berg RA, Sutton RM, Holubkov R, Nicholson CE, Dean JM, Harrison R, Heidemann S, Meert K, Newth C, Moler F, et al. Eunice Kennedy Shriver National Institute of Child Health and Human Development Collaborative Pediatric Critical Care Research Network and for the American Heart Association’s Get With the Guidelines-Resuscitation (formerly the National Registry of Cardiopulmonary Resuscitation) Investigators. Ratio of PICU versus ward cardiopulmonary resuscitation events is increasing. Crit Care Med. 2013;41:2292–2297. - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
