

Incidence, nature, and temporal trends of adverse events associated with noncardiac procedures among veterans with drug-eluting coronary artery stents
- PMID: 25323046
- PMCID: PMC4476539
- DOI: 10.1002/ccd.25706
Incidence, nature, and temporal trends of adverse events associated with noncardiac procedures among veterans with drug-eluting coronary artery stents
Abstract
Background: The incidence of adverse events with noncardiac procedures (NCP) after the use of drug eluting stents (DES) is not well studied. We sought to determine the incidence and temporal trends of adverse events in patients undergoing NCP after coronary DES.
Methods: We performed a retrospective review of patients receiving DES during percutaneous coronary intervention (PCI) in the Lexington VAMC between January 1, 2004 and December 31, 2010 to determine the circumstances and the results of their NCP.
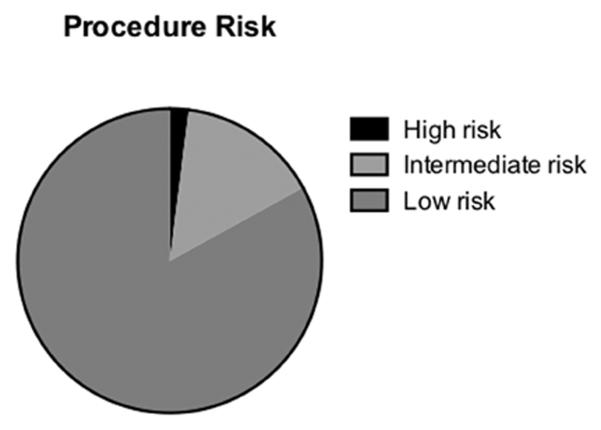
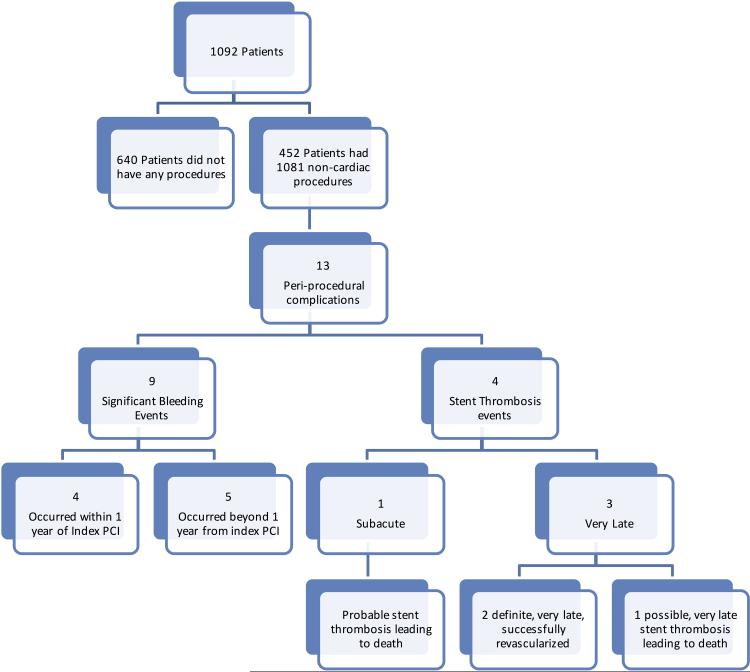
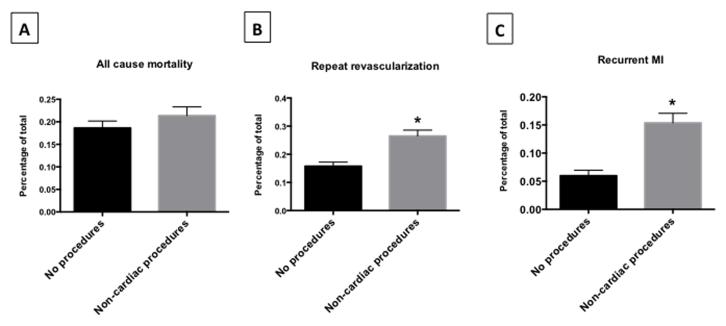
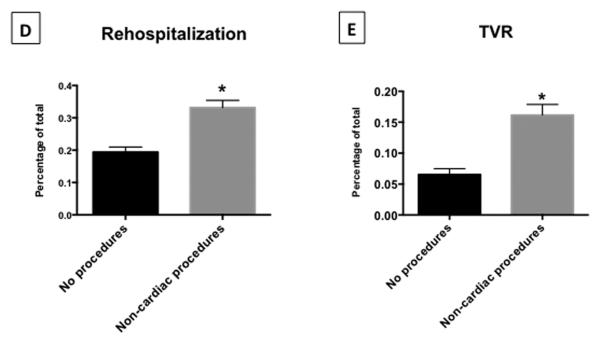
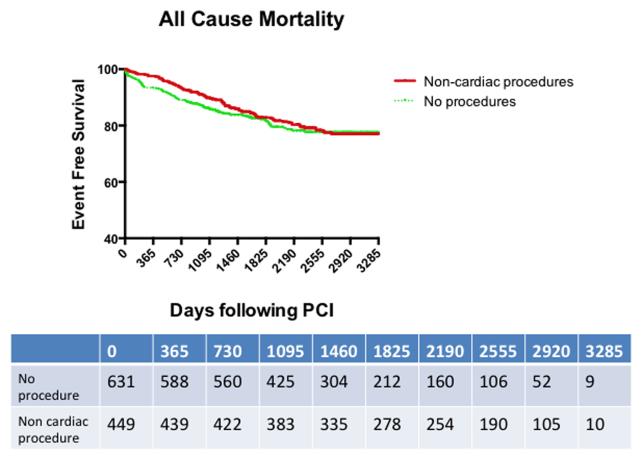
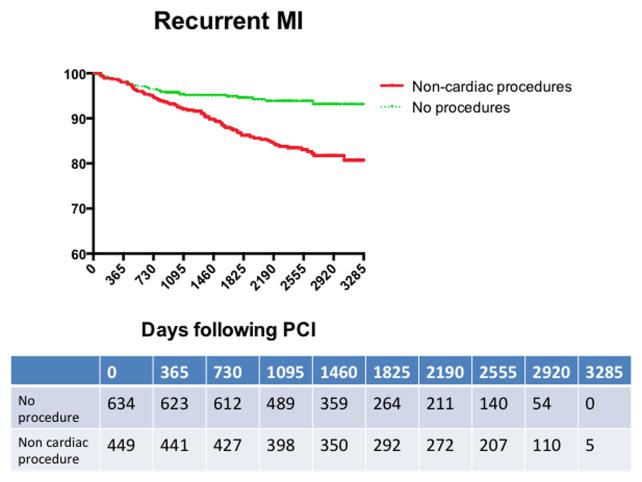
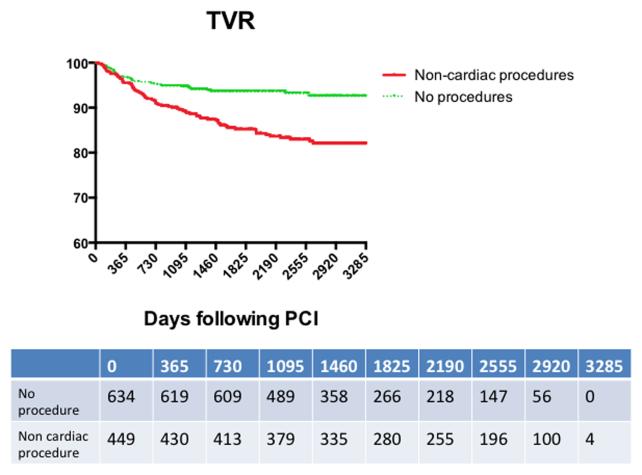
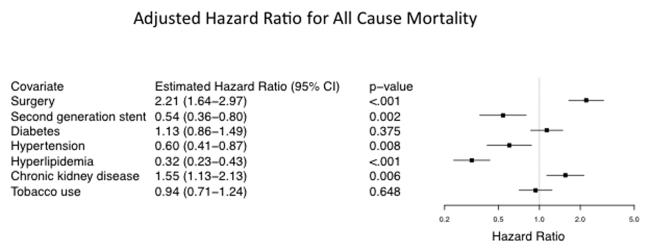
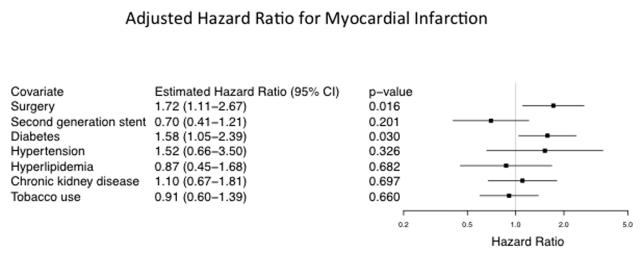
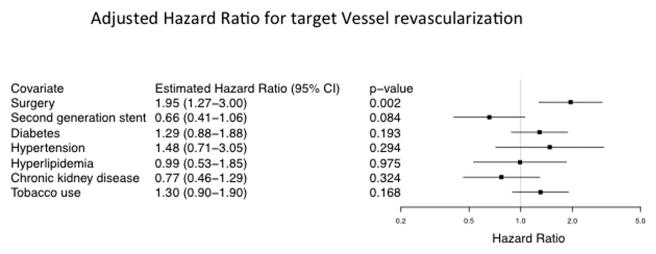
Results: We identified 1,092 patients who underwent at least one PCI with DES who were followed for at least 3 years. Of those, 452 patients (41%) had a NCP at a median of 534 days after PCI with 1,081 procedures (894 low-, 160 Intermediate-, and 27 high-risk) performed. Clinically relevant NCP-related complications were defined as significant bleeding or stent thrombosis and occurred in 13 individuals (nine perioperative bleeding and four probable/possible stent thrombosis including two mortalities). Five adverse events occurred within the first year at a rate of 0.014 event/patient-year. During the remainder of follow-up (up to 9 years), eight events were documented at a rate of 0.0004 event/patient-years. During the first year of follow-up, there was no significant increase in risk of recurrent myocardial infarction (MI) or target vessel revascularization (TVR) in patients undergoing NCP but higher risk of all-cause mortality in those who did not undergo NCP. However, in patients who underwent NCP, there was a statistically significant increase in myocardial infarction (MI), target vessel revascularization (TVR), and rehospitalization for cardiac reasons compared with those without NCP during long term follow-up (median of 5.6 years).
Conclusion: NCP after DES requiring management of DAT are relatively common among veterans following PCI using DES. The risk of bleeding and stent thrombosis is concentrated in the first year but remains very low.
Keywords: adverse events; drug eluting stents; dual antiplatelet therapy; noncardiac procedures; percutaneous coronary intervention.
© 2015 Wiley Periodicals, Inc.
Figures
Comment in
-
Non-cardiac procedures after DES: an everyday issue awaiting answers.Catheter Cardiovasc Interv. 2015 Aug;86(2):220. doi: 10.1002/ccd.26086. Catheter Cardiovasc Interv. 2015. PMID: 26198062
References
-
- Takayama T, Hiro T, Hirayama A. Stent thrombosis and drug-eluting stents. Journal of cardiology. 2011;58:92–98. - PubMed
-
- Iakovou I, Schmidt T, Bonizzoni E, et al. INcidence, predictors, and outcome of thrombosis after successful implantation of drug-eluting stents. JAMA. 2005;293:2126–2130. - PubMed
-
- Jeremias A, Sylvia B, Bridges J, et al. Stent Thrombosis After Successful Sirolimus-Eluting Stent Implantation. Circulation. 2004;109:1930–1932. - PubMed
-
- Spertus JA, Kettelkamp R, Vance C, et al. Prevalence, Predictors, and Outcomes of Premature Discontinuation of Thienopyridine Therapy After Drug-Eluting Stent Placement: Results From the PREMIER Registry. Circulation. 2006;113:2803–2809. - PubMed
-
- Airoldi F, Colombo A, Morici N, et al. Incidence and Predictors of Drug-Eluting Stent Thrombosis During and After Discontinuation of Thienopyridine Treatment. Circulation. 2007;116:745–754. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
