

The effect of folate fortification on folic acid-based homocysteine-lowering intervention and stroke risk: a meta-analysis
- PMID: 25323814
- PMCID: PMC10271370
- DOI: 10.1017/S1368980014002134
The effect of folate fortification on folic acid-based homocysteine-lowering intervention and stroke risk: a meta-analysis
Abstract
Objective: Folate and vitamin B12 are two vital regulators in the metabolic process of homocysteine, which is a risk factor of atherothrombotic events. Low folate intake or low plasma folate concentration is associated with increased stroke risk. Previous randomized controlled trials presented discordant findings in the effect of folic acid supplementation-based homocysteine lowering on stroke risk. The aim of the present review was to perform a meta-analysis of relevant randomized controlled trials to check the how different folate fortification status might affect the effects of folic acid supplementation in lowering homocysteine and reducing stroke risk.
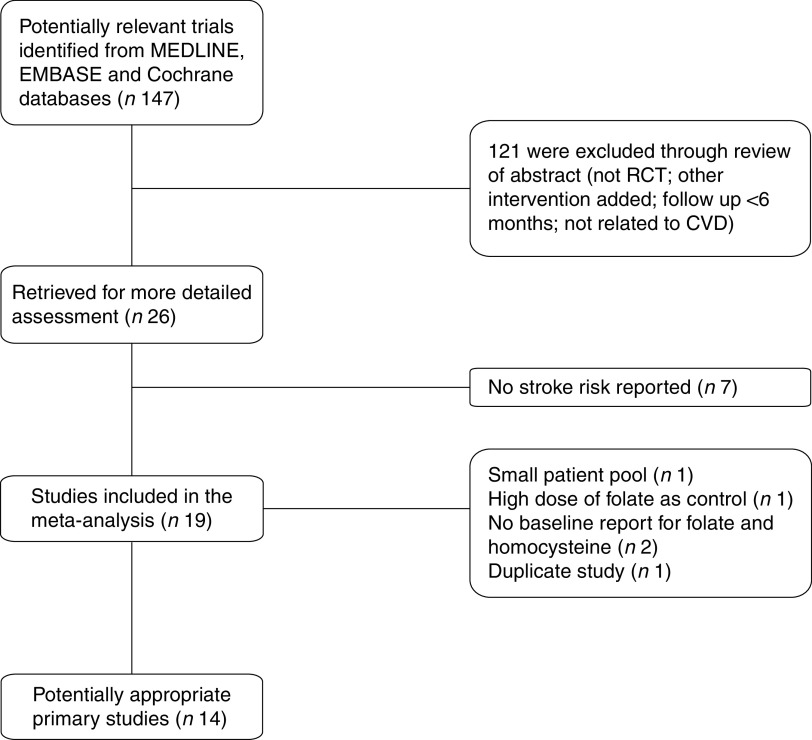
Design: Relevant randomized controlled trials were identified through formal literature search. Homocysteine reduction was compared in subgroups stratified by folate fortification status. Relative risks with 95 % confidence intervals were used as a measure to assess the association between folic acid supplementation and stroke risk.
Setting: The meta-analysis included fourteen randomized controlled trials,
Subjects: A total of 39 420 patients.
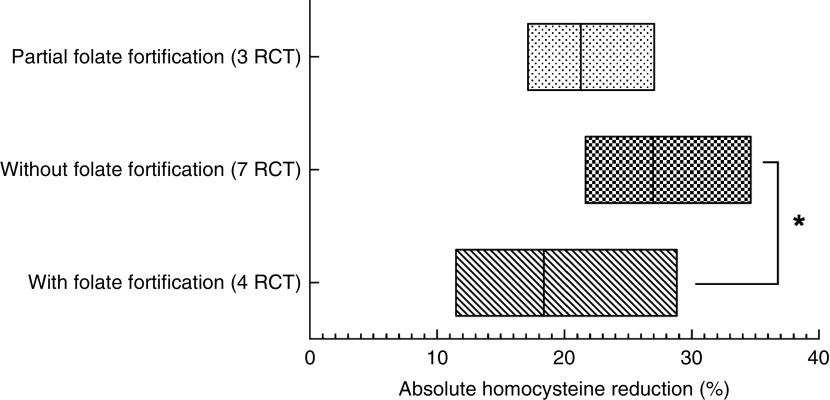
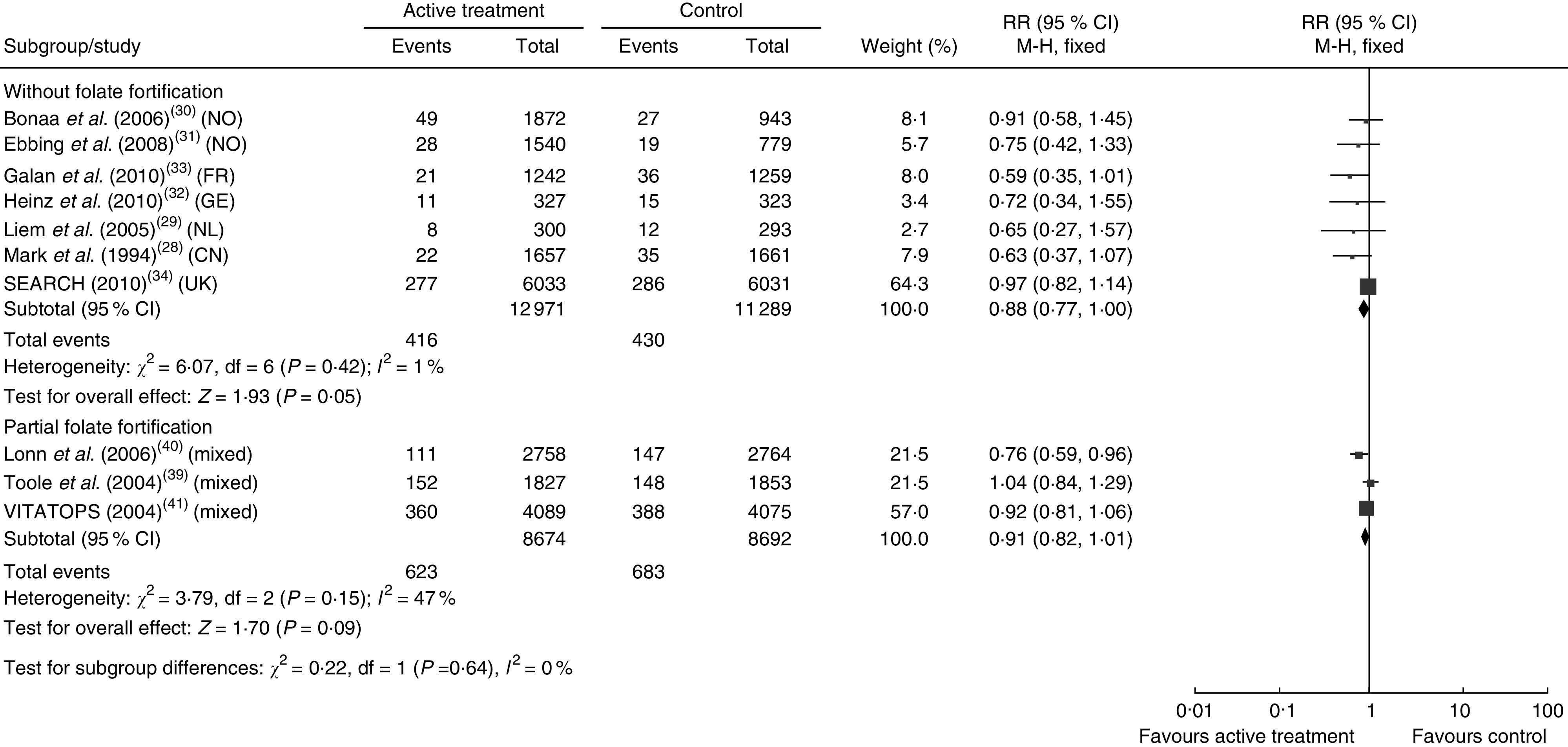
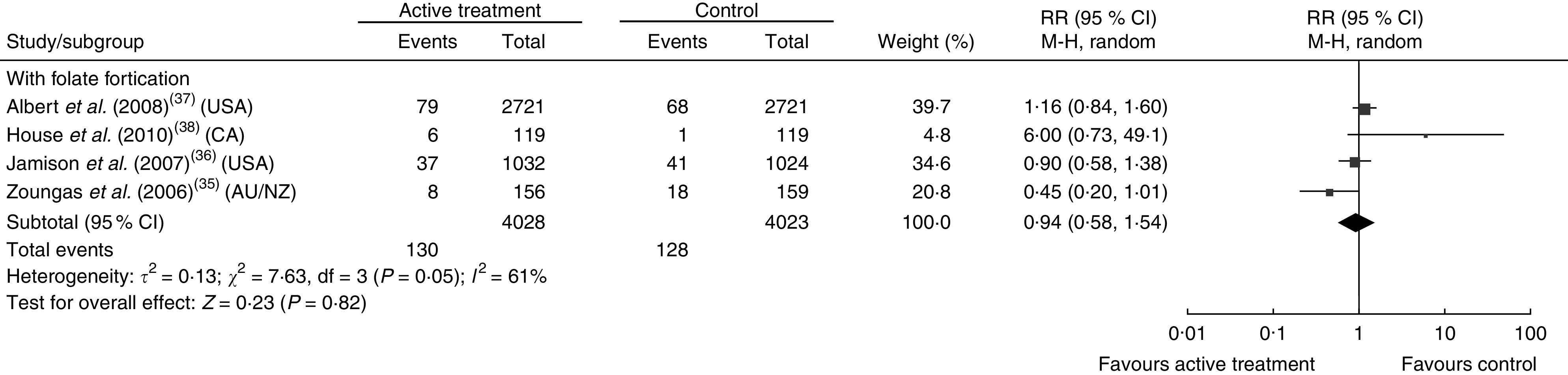
Results: Homocysteine reductions were 26·99 (sd 1·91) %, 18·38 (sd 3·82) % and 21·30 (sd 1·98) %, respectively, in the subgroups without folate fortification, with folate fortification and with partial folate fortification. Significant difference was observed between the subgroups with folate fortification and without folate fortification (P=0·05). The relative risk of stroke was 0·88 (95 % CI 0·77, 1·00, P=0·05) in the subgroup without folate fortification, 0·94 (95 % CI 0·58, 1·54, P=0·82) in the subgroup with folate fortification and 0·91 (95 % CI 0·82, 1·01, P=0·09) in the subgroup with partial folate fortification.
Conclusions: Folic acid supplementation might have a modest benefit on stroke prevention in regions without folate fortification.
Keywords: Folate fortification.
Figures
References
-
- Guthikonda S & Haynes WG (2006) Homocysteine: role and implications in atherosclerosis. Curr Atheroscler Rep 8, 100–106. - PubMed
-
- Ridker PM, Manson JE, Buring JE et al.. (1999) Homocysteine and risk of cardiovascular disease among postmenopausal women. JAMA 281, 1817–1821. - PubMed
-
- Lawson MF (1998) Homocysteine and atherothrombosis. N Engl J Med 339, 477–478; author reply 479. - PubMed
-
- Curro M, Condello S, Caccamo D et al.. (2009) Homocysteine-induced toxicity increases TG2 expression in Neuro2a cells. Amino Acids 36, 725–730. - PubMed
-
- Yap S, Rushe H, Howard PM et al.. (2001) The intellectual abilities of early-treated individuals with pyridoxine-nonresponsive homocystinuria due to cystathionine β-synthase deficiency. J Inherit Metab Dis 24, 437–447. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
