

Current treatments in familial dysautonomia
- PMID: 25323828
- PMCID: PMC4236240
- DOI: 10.1517/14656566.2014.970530
Current treatments in familial dysautonomia
Abstract
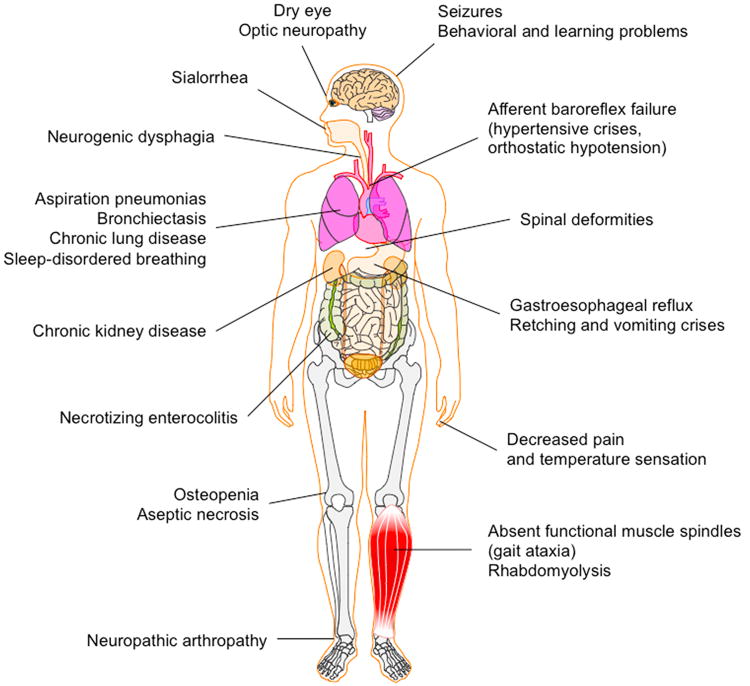
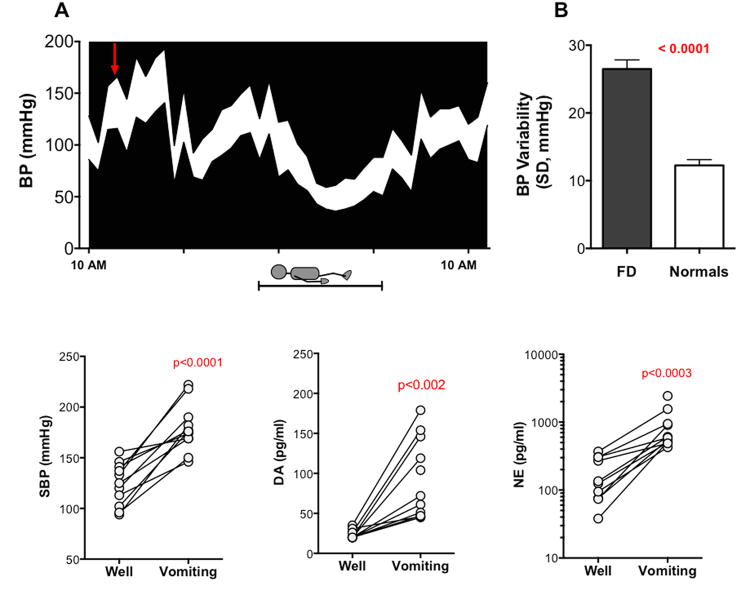
Introduction: Familial dysautonomia (FD) is a rare hereditary sensory and autonomic neuropathy (type III). The disease is caused by a point mutation in the IKBKAP gene that affects the splicing of the elongator-1 protein (ELP-1) (also known as IKAP). Patients have dramatic blood pressure instability due to baroreflex failure, chronic kidney disease, and impaired swallowing leading to recurrent aspiration pneumonia, which results in chronic lung disease. Diminished pain and temperature perception result in neuropathic joints and thermal injuries. Impaired proprioception leads to gait ataxia. Optic neuropathy and corneal opacities lead to progressive visual loss.
Areas covered: This article reviews current therapeutic strategies for the symptomatic treatment of FD, as well as the potential of new gene-modifying agents.
Expert opinion: Therapeutic focus on FD is centered on reducing the catecholamine surges caused by baroreflex failure. Managing neurogenic dysphagia with effective protection of the airway passages and prompt treatment of aspiration pneumonias is necessary to prevent respiratory failure. Sedative medications should be used cautiously due to the risk of respiratory depression. Non-invasive ventilation during sleep effectively manages apneas and prevents hypercapnia. Clinical trials of compounds that increase levels of IKAP (ELP-1) are underway and will determine whether they can reverse or slow disease progression.
Keywords: future directions; hereditary autonomic neuropathy; hypertensive surges; nausea; splicing modification therapy.
Conflict of interest statement
LNK: receives research support from the National Institutes of Health (U54NS065736) and the Dysautonomia Foundation, Inc.
CFM: receives research support from the Dysautonomia Foundation, Inc.
CMS: receives research support from the Dysautonomia Foundation, Inc.
LP: receives research support from the Dysautonomia Foundation, Inc.
HK: serves receives research support from the National Institutes of Health (U54NS065736 [PI]) 1U01NS078025-01, the FDA (FD-R-3731-01 [PI]), and the Dysautonomia Foundation, Inc; has received compensation as a consultant/advisory board member for Lundbeck, Eli Lilly, Pfizer, and Astra Zeneca.
Figures


References
-
- Riley CM, Day RL, et al. Central autonomic dysfunction with defective lacrimation; report of five cases. Pediatrics. 1949 Apr;3(4):468–78. The first description of familial dysautonomia by Riley and Day. - PubMed
-
- Blumenfeld A, Slaugenhaupt SA, Axelrod FB, et al. Localization of the gene for familial dysautonomia on chromosome 9 and definition of DNA markers for genetic diagnosis. Nat Genet. 1993 Jun;4(2):160–4. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical