

Clinical pathways for fragility fractures of the pelvic ring: personal experience and review of the literature
- PMID: 25323921
- PMCID: PMC4306730
- DOI: 10.1007/s00776-014-0653-9
Clinical pathways for fragility fractures of the pelvic ring: personal experience and review of the literature
Abstract
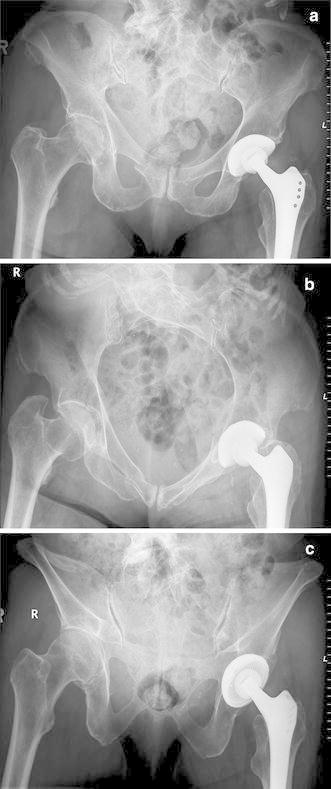
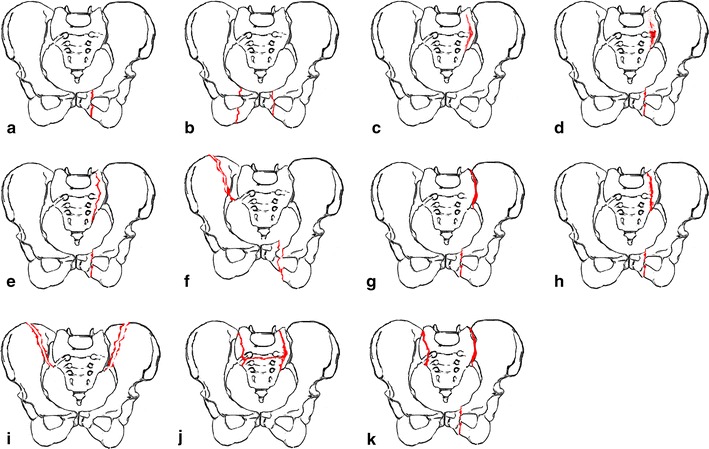
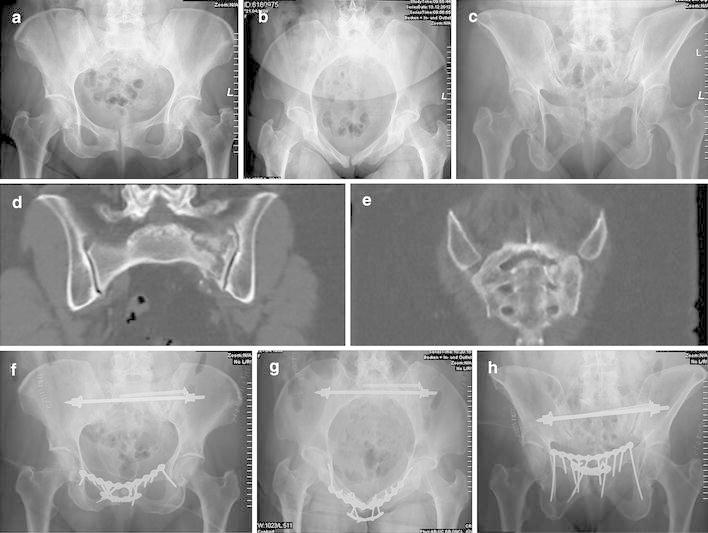
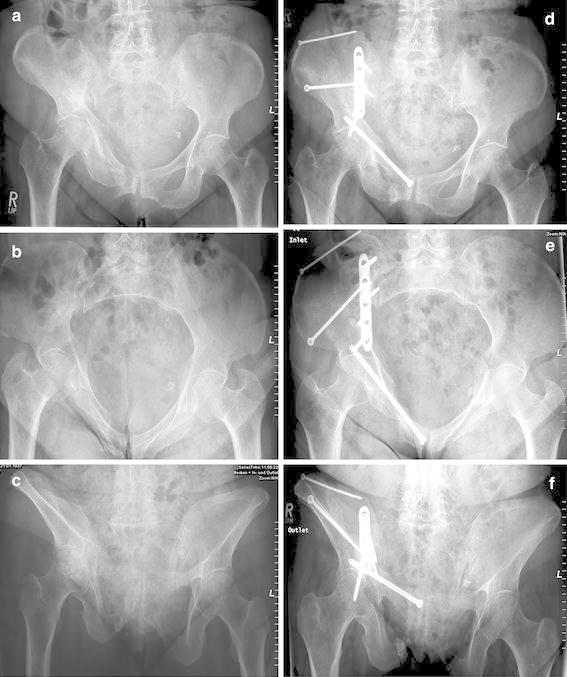
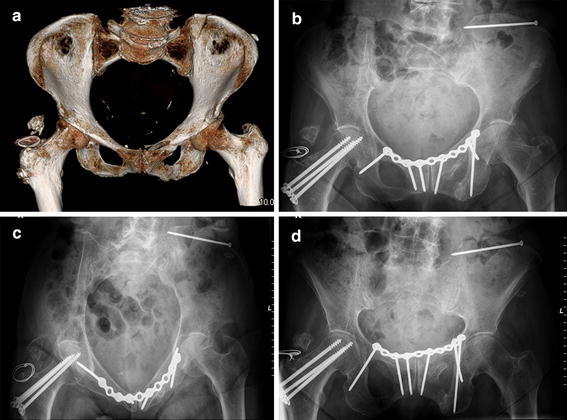
Fragility fractures of the pelvic ring (FFP) are increasing in frequency and require challenging treatment. A new comprehensive classification considers both fracture morphology and degree of instability. The classification system also provides recommendations for type and invasiveness of treatment. In this article, a literature review of treatment alternatives is presented and compared with our own experiences. Whereas FFP Type I lesions can be treated conservatively, FFP Types III and IV require surgical treatment. For FFP Type II lessions, percutaneous fixation techniques should be considered after a trial of conservative treatment. FFP Type III lesions need open reduction and internal fixation, whereas FFP Type IV lesions require bilateral fixation. The respective advantages and limitations of dorsal (sacroiliac screw fixation, sacroplasty, bridging plate fixation, transsacral positioning bar placement, angular stable plate) and anterior (external fixation, angular stable plate fixation, retrograde transpubic screw fixation) pelvic fixations are described.
Figures



References
-
- Kates SL, Bukata SV, DiGiovanni BF, Friedman SM, Hoyen H, Kates A, Kates SL, Mears SC, Mendelson DA, Serna FH, Jr., Sieber FE and Tyler WK. A guide to improving the care of patients with fragility fractures. Geriatric orthopaedic surgery and rehabilitation 2011; 2: 5-37. http://gos.sagepub.com/content/2/1/5. - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
