

Complications related to gastric endoscopic submucosal dissection and their managements
- PMID: 25324997
- PMCID: PMC4198554
- DOI: 10.5946/ce.2014.47.5.398
Complications related to gastric endoscopic submucosal dissection and their managements
Abstract
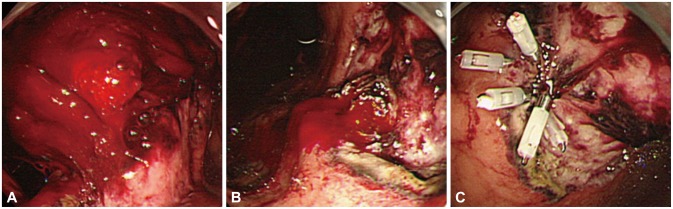
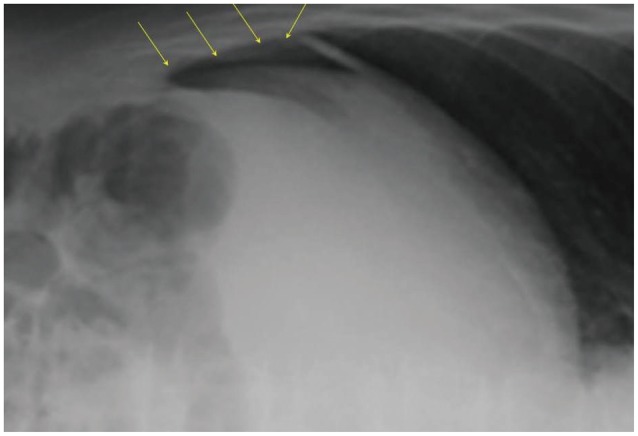
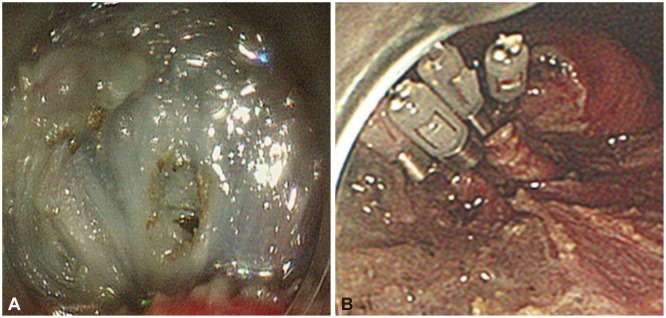
Endoscopic submucosal dissection (ESD) for early gastric cancer is a well-established procedure with the advantage of resection in an en bloc fashion, regardless of the size, shape, coexisting ulcer, and location of the lesion. However, gastric ESD is a more difficult and meticulous technique, and also requires a longer procedure time, than conventional endoscopic mucosal resection. These factors naturally increase the risk of various complications. The two most common complications accompanying gastric ESD are bleeding and perforation. These complications are known to occur both intraoperatively and postoperatively. However, there are other rare but serious complications related to gastric ESD, including aspiration pneumonia, stenosis, venous thromboembolism, and air embolism. Endoscopists should have sufficient knowledge about such complications and be prepared to deal with them appropriately, as successful management of complications is necessary for the successful completion of the entire ESD procedure.
Keywords: Complication; Endoscopic submucosal dissection; Hemorrhage; Perforation.
Conflict of interest statement
The authors have no financial conflicts of interest.
Figures
References
-
- Goda K, Fujishiro M, Hirasawa K, et al. How to teach and learn endoscopic submucosal dissection for upper gastrointestinal neoplasm in Japan. Dig Endosc. 2012;24(Suppl 1):136–142. - PubMed
-
- Oda I, Gotoda T, Hamanaka H, et al. Endoscopic submucosal dissection for early gastric cancer: technical feasibility, operation time and complications from a large consecutive series. Dig Endosc. 2005;17:54–58.
-
- Fujishiro M, Yahagi N, Kakushima N, et al. Management of bleeding concerning endoscopic submucosal dissection with the flex knife for stomach neoplasm. Dig Endosc. 2006;18(Suppl 1):S119–S122.
-
- Toyonaga T, Nishino E, Hirooka T, Ueda C, Noda K. Intraoperative bleeding in endoscopic submucosal dissection in the stomach and strategy for prevention and treatment. Dig Endosc. 2006;18(Suppl 1):S123–S127.
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
