

Neoplasia in chronic pancreatitis: how to maximize the yield of endoscopic ultrasound-guided fine needle aspiration
- PMID: 25325001
- PMCID: PMC4198558
- DOI: 10.5946/ce.2014.47.5.420
Neoplasia in chronic pancreatitis: how to maximize the yield of endoscopic ultrasound-guided fine needle aspiration
Abstract
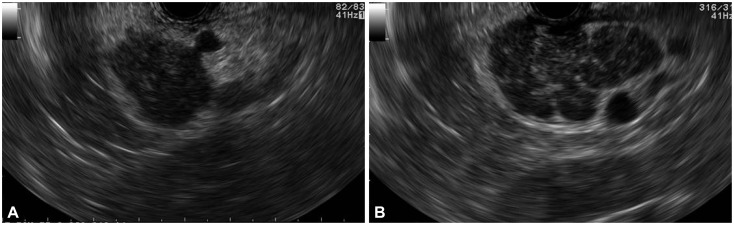
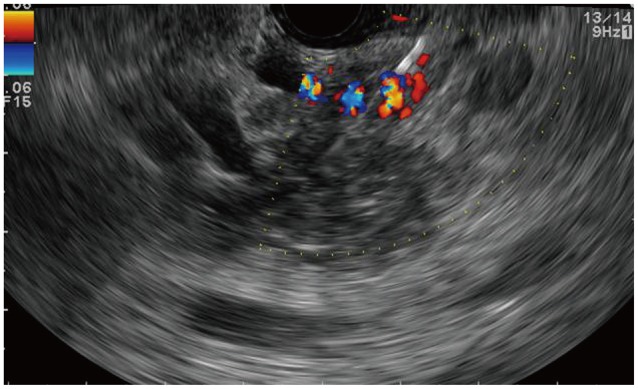
When performing endoscopic ultrasound-guided fine needle aspiration (EUS-FNA), identifying neoplasia in the setting of chronic pancreatitis can be technically challenging. The morphology of an ill-defined mass on sonography, presence of calcifications or intervening collaterals, reverberation from a biliary stent, low yield of tissue procurement, and interpretative errors in cytopathology can result in both false-negative and false-positive results. Although these challenges cannot be completely eliminated, elastography or contrast-enhanced imaging can aid in differentiating an inflammatory mass from a neoplasm. Also, performing more passes of FNA, procuring core biopsy material, performing rapid onsite evaluation, conducting ancillary pathology studies, and even repeating the procedure on a different day can aid in improving the diagnostic performance of EUS-FNA. This review provides a concise update and offers practical tips to improving the diagnostic yield of EUS-FNA when sampling solid pancreatic mass lesions in the setting of chronic pancreatitis.
Keywords: Biopsy; Biopsy, fine-needle; Endosonography; Pancreatic neoplasms; Pancreatitis, chronic.
Conflict of interest statement
The authors have no financial conflicts of interest.
Figures

References
-
- Fritscher-Ravens A, Brand L, Knöfel WT, et al. Comparison of endoscopic ultrasound-guided fine needle aspiration for focal pancreatic lesions in patients with normal parenchyma and chronic pancreatitis. Am J Gastroenterol. 2002;97:2768–2775. - PubMed
-
- Varadarajulu S, Tamhane A, Eloubeidi MA. Yield of EUS-guided FNA of pancreatic masses in the presence or the absence of chronic pancreatitis. Gastrointest Endosc. 2005;62:728–736. - PubMed
-
- Kulesza P, Eltoum IA. Endoscopic ultrasound-guided fine-needle aspiration: sampling, pitfalls, and quality management. Clin Gastroenterol Hepatol. 2007;5:1248–1254. - PubMed
-
- Frey H. Realtime elastography. A new ultrasound procedure for the reconstruction of tissue elasticity. Radiologe. 2003;43:850–855. - PubMed
-
- Saftoiu A, Vilman P. Endoscopic ultrasound elastography: a new imaging technique for the visualization of tissue elasticity distribution. J Gastrointestin Liver Dis. 2006;15:161–165. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
