

An evidence-based recommendation for a new definition of respiratory-related leg movements
- PMID: 25325500
- PMCID: PMC4288611
- DOI: 10.5665/sleep.4418
An evidence-based recommendation for a new definition of respiratory-related leg movements
Abstract
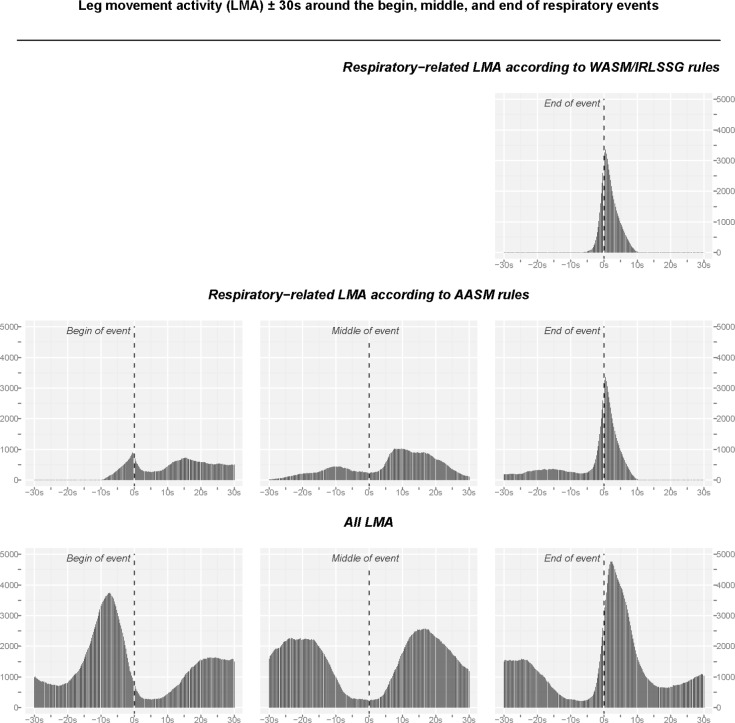
Study objectives: Current sleep scoring rules exclude leg movements that occur near respiratory events from being scored as periodic leg movements during sleep (PLMS) but differ in whether they exclude leg movements occurring at the end (WASM/ IRLSSG) or during a respiratory event (AASM). The aim of the present study was to describe the distribution of leg movements in relation to respiratory events and to contribute to an evidence-based rule for the identification and scoring of respiratory-related leg movements (RRLMs).
Design: Retrospective chart review and analysis of polysomnographic recordings.
Setting: Clinical sleep laboratory.
Participants: 64 patients with polysomnographic recordings between January 2010 and July 2011, aged 18 to 75 years, with AHI >20, ODI >10, more than 50% of apneas being obstructive, >15 leg movements of any type per hour of sleep, no more than 20% of total sleep time with artifacts and no medical condition or medication that could influence leg movements or respiratory disturbances.
Interventions: None.
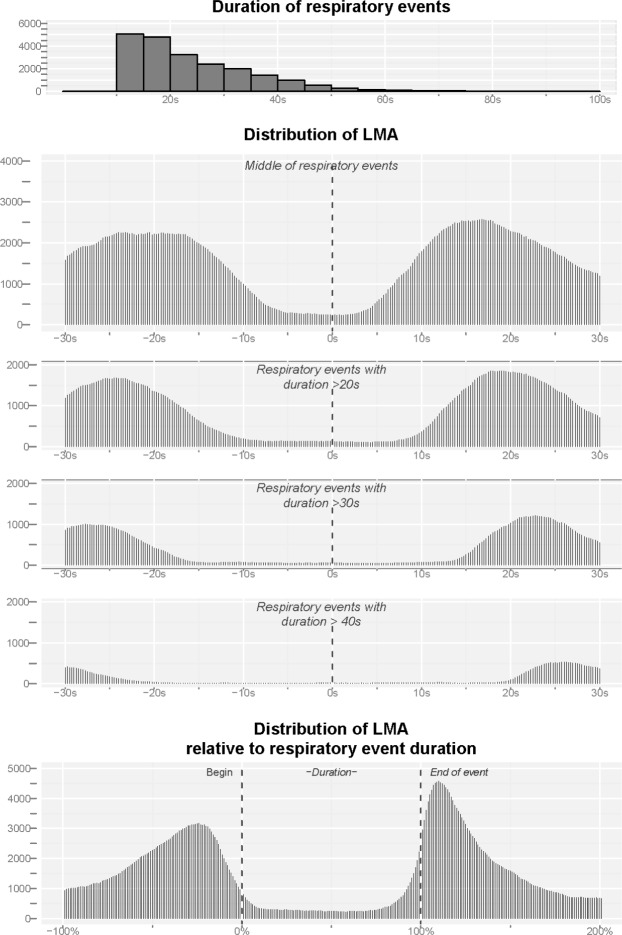
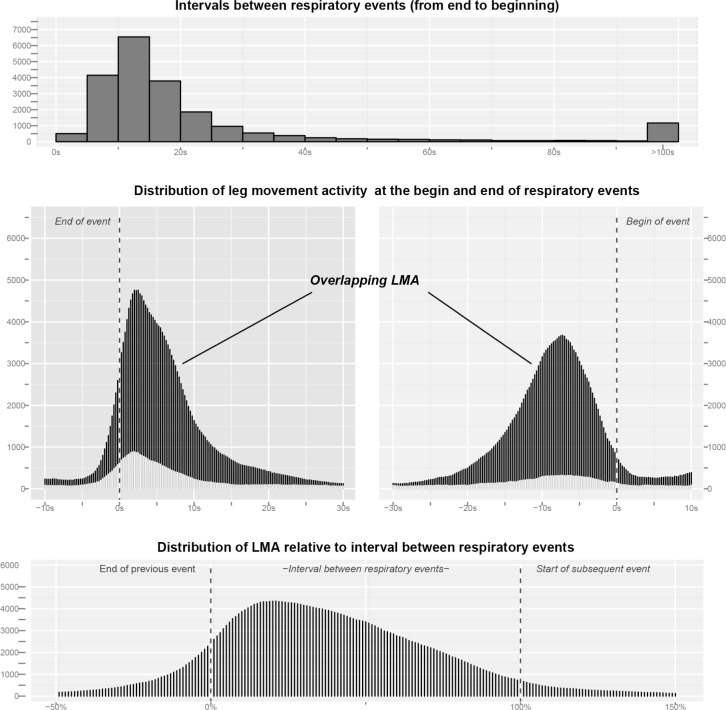
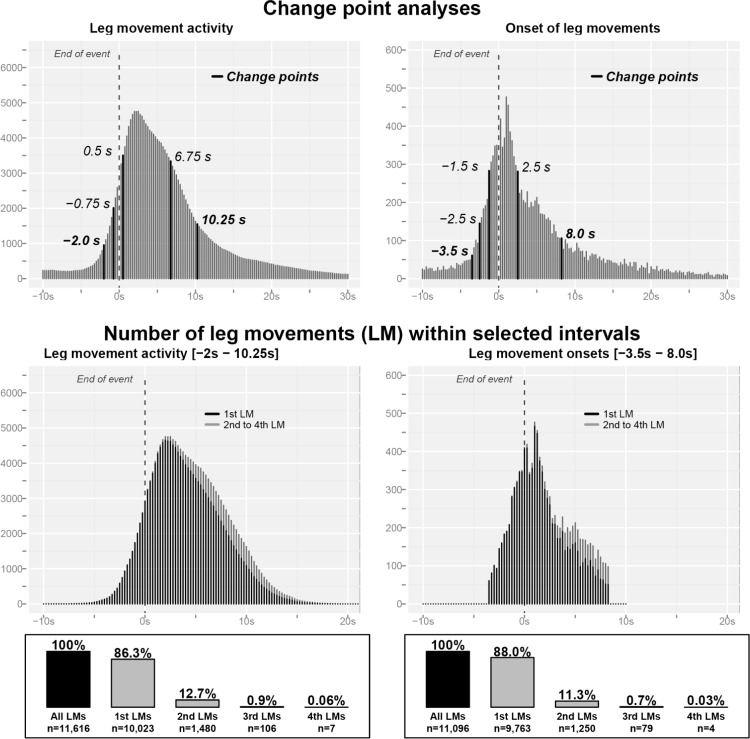
Measurements and results: Back-averaging of leg movement activity (LMA) with respect to respiratory events revealed that LMA was present shortly before the end of the respiratory events, but occurred mostly following respiratory events with peak onset of LMA 2.5 s after respiratory event termination. Increased LMA before the beginning of the respiratory event consisted mainly of the tail of LMA after the end of the previous respiratory event. Change-point analysis indicated that LMA was increased over an interval of -2.0 s to +10.25 s around the end of respiratory events. Changing the definition of RRLMs had a significant influence on PLMS counts. The number of patients with obstructive sleep apnea (OSA) with PLMS index >15 was 80% when considering the WASM/ IRLSSG definition, 67% for the AASM criteria, and 41% when based on the interval identified by change-point analysis (-2.0 to 10.25 s).
Conclusions: Leg movements are not augmented at the beginning or middle of respiratory events but are increased around the end of respiratory events over a period significantly longer than specified in the AASM and the WASM/ IRLSSG rules. Both rules underestimate the number of RRLMs and thus overestimate the number of PLMS in patients with OSA.
Keywords: Respiratory-related leg movements; periodic leg movements; sleep apnea.
© 2015 Associated Professional Sleep Societies, LLC.
Figures
References
-
- Iber C, Ancoli-Israel S, Chesson A, Quan S American Academy of Sleep Medicine. 1st ed. Westchester, IL: American Academy of Sleep Medicine; 2007. The AASM manual for the scoring of sleep and associated events: rules, terminology and technical specifications.
-
- Ferri R. The time structure of leg movement activity during sleep: the theory behind the practice. Sleep Med. 2012;13:433–41. - PubMed
-
- Hornyak M, Feige B, Riemann D, Voderholzer U. Periodic leg movements in sleep and periodic limb movement disorder: prevalence, clinical significance and treatment. Sleep Med Rev. 2006;10:169–77. - PubMed
-
- Olson EJ, Boeve BF, Silber MH. Rapid eye movement sleep behaviour disorder: demographic, clinical and laboratory findings in 93 cases. Brain. 2000;123:331–9. - PubMed
-
- Dauvilliers Y, Pennestri MH, Petit D, Dang-Vu T, Lavigne G, Montplaisir J. Periodic leg movements during sleep and wakefulness in narcolepsy. J Sleep Res. 2007;16:333–9. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
