

Efficacy of home single-channel nasal pressure for recommending continuous positive airway pressure treatment in sleep apnea
- PMID: 25325508
- PMCID: PMC4262946
- DOI: 10.5665/sleep.4316
Efficacy of home single-channel nasal pressure for recommending continuous positive airway pressure treatment in sleep apnea
Abstract
Introduction: Unlike other prevalent diseases, obstructive sleep apnea (OSA) has no simple tool for diagnosis and therapeutic decision-making in primary healthcare. Home single-channel nasal pressure (HNP) may be an alternative to polysomnography for diagnosis but its use in therapeutic decisions has yet to be explored.
Objectives: To ascertain whether an automatically scored HNP apnea-hypopnea index (AHI), used alone to recommend continuous positive airway pressure (CPAP) treatment, agrees with decisions made by a specialist using polysomnography and several clinical variables.
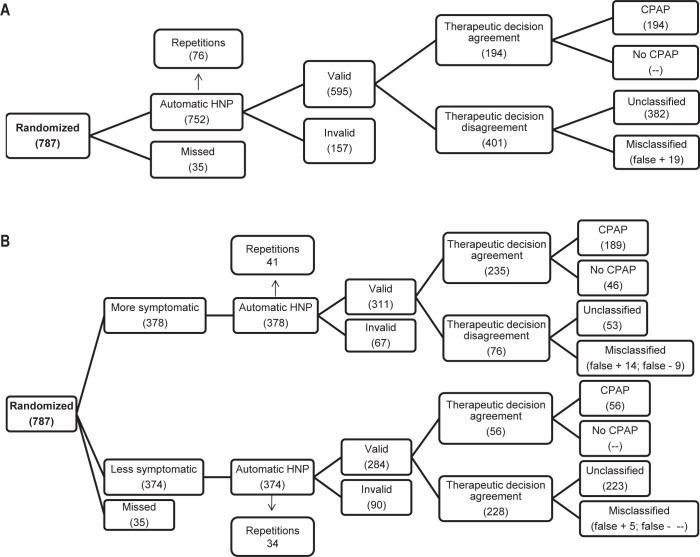
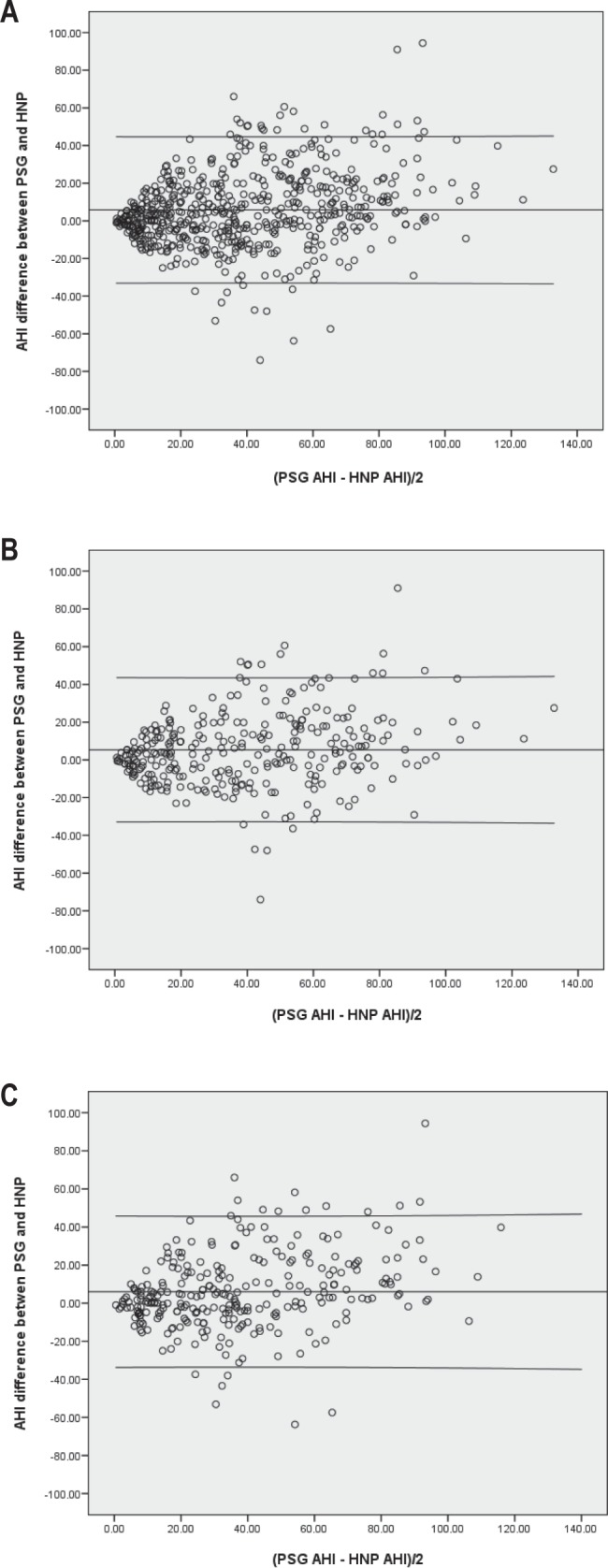
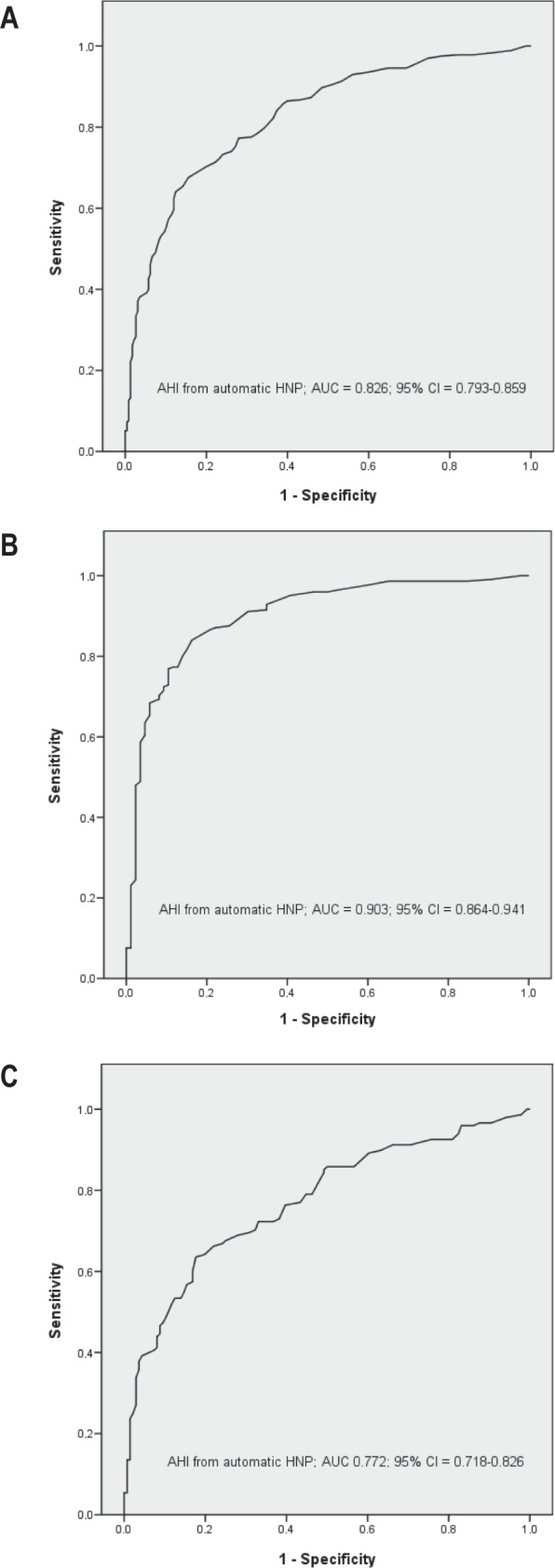
Methods: Patients referred by primary care physicians for OSA suspicion underwent randomized polysomnography and HNP. We analyzed the total sample and both more and less symptomatic subgroups for Bland and Altman plots to explore AHI agreement; receiver operating characteristic curves to establish area under the curve (AUC) measurements for CPAP recommendation; and therapeutic decision efficacy for several HNP AHI cutoff points.
Results: Of the 787 randomized patients, 35 (4%) were lost, 378 (48%) formed the more symptomatic and 374 (48%) the less symptomatic subgroups. AHI bias and agreement limits were 5.8 ± 39.6 for the total sample, 5.3 ± 38.7 for the more symptomatic, and 6 ± 40.2 for the less symptomatic subgroups. The AUC were 0.826 for the total sample, 0.903 for the more symptomatic, and 0.772 for the less symptomatic subgroups. In the more symptomatic subgroup, 70% of patients could be correctly treated with CPAP.
Conclusion: Automatic HNP scoring can correctly recommend CPAP treatment in most of more symptomatic patients with OSA suspicion. Our results suggest that this device may be an interesting tool in initial OSA management for primary care physicians, although future studies in a primary care setting are necessary.
Clinical trials information: Clinicaltrial.gov identifier: NCT01347398.
Keywords: Apnealink; CPAP; portable monitor; sleep apnea.
© 2014 Associated Professional Sleep Societies, LLC.
Figures
Comment in
-
Are we ready for "unisomnography"?Sleep. 2015 Jan 1;38(1):7-9. doi: 10.5665/sleep.4312. Sleep. 2015. PMID: 25515113 Free PMC article. No abstract available.
References
-
- Durán J, Esnaola S, Rubio R, et al. Obstructive sleep apnea-hypopnea and related clinical features in a population-based sample of subjects aged 30 to 70 yr. Am J Respir Crit Care Med. 2001;163:685–9. - PubMed
-
- Ballester E, Badia JR, Hernández L, et al. Evidence of the effectiveness of continuous positive airway pressure in the treatment of sleep apnea/ hypopnea syndrome. Am J Respir Crit Care Med. 1999;159:495–501. - PubMed
-
- Marin JM, Carrizo SJ, Vicente E, et al. Long-term cardiovascular outcomes in men with obstructive sleep apnoea-hypopnoea with or without treatment with continuous positive airway pressure: an observational study. Lancet. 2005;365:1046–53. - PubMed
-
- Barbé F, Durán-Cantolla J, Sánchez-de-la-Torre M, et al. Spanish Sleep and Breathing Network. Effect of continuous positive airway pressure on the incidence of hypertension and cardiovascular events in nonsleepy patients with obstructive sleep apnea: a randomized controlled trial. JAMA. 2012;307:2161–8. - PubMed
-
- Terán-Santos J, Jiménez-Gómez A, Cordero-Guevara J, et al. The association between sleep apnea and the risk of traffic accidents. Cooperative Group Burgos-Santander. N Engl J Med. 1999;340:847–51. - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
