

Mobile health, exercise and metabolic risk: a randomized controlled trial
- PMID: 25326074
- PMCID: PMC4210561
- DOI: 10.1186/1471-2458-14-1082
Mobile health, exercise and metabolic risk: a randomized controlled trial
Abstract
Background: It was hypothesized that a mobile health (mHealth) intervention would elicit greater improvements in systolic blood pressure and other cardiometabolic risk factors at 12 weeks, which would be better maintained over 52 weeks, compared to the active control intervention.
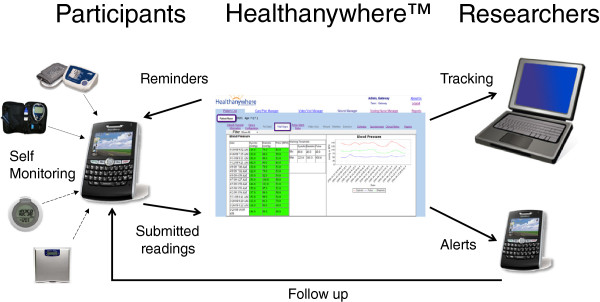
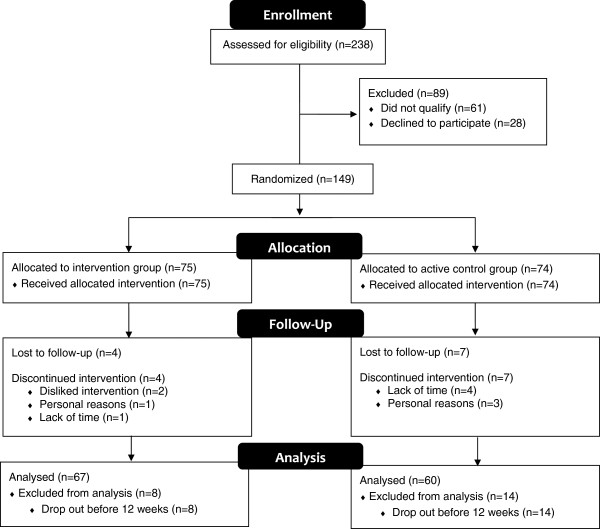
Methods: Eligible participants (≥2 metabolic syndrome risk factors) were randomized to the mHealth intervention (n = 75) or the active control group (n = 74). Blood pressure and other cardiometabolic risk factors were measured at baseline and at 12, 24 and 52 weeks. Both groups received an individualized exercise prescription and the intervention group additionally received a technology kit for home monitoring of biometrics and physical activity.
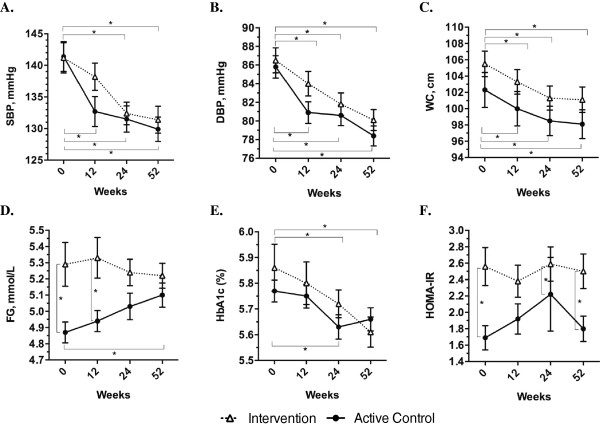
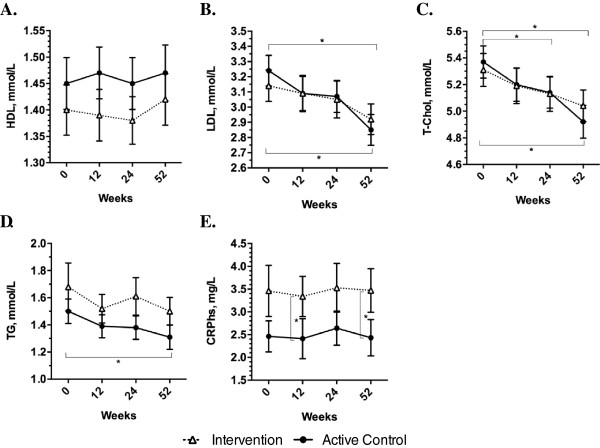
Results: Analyses were conducted on 67 participants in the intervention group (aged 56.7 ± 9.7 years; 71.6% female) and 60 participants in the active control group (aged 59.1 ± 8.4 years; 76.7% female). At 12 weeks, baseline adjusted mean change in systolic blood pressure (primary outcome) was greater in the active control group compared to the intervention group (-5.68 mmHg; 95% CI -10.86 to -0.50 mmHg; p = 0.03), but there were no differences between groups in mean change for secondary outcomes. Over 52-weeks, the difference in mean change for systolic blood pressure was no longer apparent between groups, but remained significant across the entire population (time: p < 0.001).
Conclusions: In participants with increased cardiometabolic risk, exercise prescription alone had greater short-term improvements in systolic blood pressure compared to the mHealth intervention, though over 52 weeks, improvements were equal between interventions.
Trial registration: ClinicalTrials.gov http://NCT01944124.
Figures
References
-
- Mendis S, Puska P, Norrving B, editors. Global Atlas on Cardiovascular Disease Prevention and Control. Geneva, Switzerland: World Health Organization; 2011.
-
- Alberti KGMM, Eckel RH, Grundy SM, Zimmet PZ, Cleeman JI, Donato KA, Fruchart JC, James WP, Loria CM, Smith SC., Jr Harmonizing the metabolic syndrome: A joint interim statement of the International Diabetes Federation task force on epidemiology and prevention; National Heart, Lung, and Blood Institute; American Heart Association; World Heart Federation; International Atherosclerosis Society; and International Association for the Study of Obesity. Circulation. 2009;120(16):1640–1645. doi: 10.1161/CIRCULATIONAHA.109.192644. - DOI - PubMed
-
- Leiter LA, Fitchett DH, Gilbert RE, Gupta M, Mancini GB, McFarlane PA, Ross R, Teoh H, Verma S, Anand S, Camelon K, Chow CM, Cox JL, Després JP, Genest J, Harris SB, Lau DC, Lewanczuk R, Liu PP, Lonn EM, McPherson R, Poirier P, Qaadri S, Rabasa-Lhoret R, Rabkin SW, Sharma AM, Steele AW, Stone JA, Tardif JC, Cardiometabolic Risk Working Group: Executive Committee et al. Cardiometabolic risk in canada: A detailed analysis and position paper by the cardiometabolic risk working group. Can J Cardiol. 2011;27(2):e1–e33. doi: 10.1016/j.cjca.2010.12.054. - DOI - PubMed
-
- Statistics Canada: 2010 health profile.http://www12.statcan.gc.ca
Pre-publication history
-
- The pre-publication history for this paper can be accessed here:http://www.biomedcentral.com/1471-2458/14/1082/prepub
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
