

Cavitary alveolar sarcoidosis complicated by an aspergilloma
- PMID: 25326564
- PMCID: PMC4202036
- DOI: 10.1136/bcr-2014-206280
Cavitary alveolar sarcoidosis complicated by an aspergilloma
Abstract
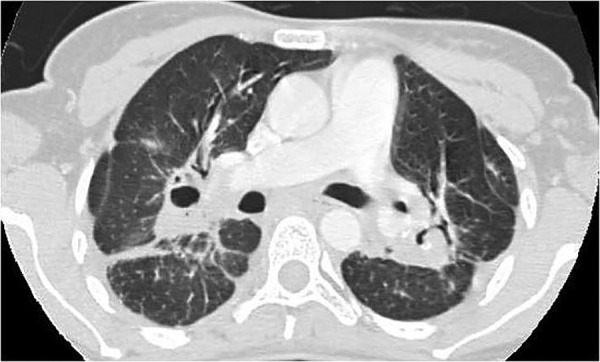
Cavitation in pulmonary sarcoidosis is rather unusual and even rarer in the alveolar form of the disease. A review of the literature revealed only 13 documented patients with cavitating alveolar sarcoidosis. Of the 13 patients, clinical information was available in only eight cases. Aspergilloma complicating cavitary alveolar sarcoidosis has been documented only once before. A 38-year-old woman with progressive dyspnoea for 3 years presented owing to a bout of haemoptysis. Imaging prior to presentation demonstrated mediastinal lymphadenopathy and coalescent parenchymal alveolar opacities along with air bronchograms, suggestive of alveolar sarcoidosis. On presentation, cavitations were visible in both lungs within the consolidation along with an intracavitary mass in the left upper lobe, which on evaluation was recognised as an aspergilloma. Bronchoscopy disclosed non-caseating granulomas on histopathology confirming pulmonary sarcoidosis. Cavitary alveolar sarcoidosis with aspergilloma formation can result in a diagnostic dilemma, especially in endemic tuberculous areas.
2014 BMJ Publishing Group Ltd.
Figures




Similar articles
-
Acute alveolar sarcoidosis presenting with hypoxaemic respiratory failure.BMJ Case Rep. 2014 Apr 30;2014:bcr2013202247. doi: 10.1136/bcr-2013-202247. BMJ Case Rep. 2014. PMID: 24789154 Free PMC article.
-
Aspergilloma formation in cavitary sarcoidosis.J Bras Pneumol. 2009 May;35(5):480-3. doi: 10.1590/s1806-37132009000500015. J Bras Pneumol. 2009. PMID: 19547859 English, Portuguese.
-
AIRP best cases in radiologic-pathologic correlation: pulmonary sarcoidosis complicated by aspergilloma formation.Radiographics. 2012 Mar-Apr;32(2):469-73. doi: 10.1148/rg.322115024. Radiographics. 2012. PMID: 22411943 Review. No abstract available.
-
Pulmonary sarcoidosis: calcified micronodular pattern simulating pulmonary alveolar microlithiasis.J Thorac Imaging. 1999 Jul;14(3):218-20. J Thorac Imaging. 1999. PMID: 10404510
-
[Three cases of primary acute pulmonary cavitation in sarcoidosis].Nihon Kokyuki Gakkai Zasshi. 2000 Dec;38(12):952-7. Nihon Kokyuki Gakkai Zasshi. 2000. PMID: 11244735 Review. Japanese.
Cited by
-
Concomitant occurrence of advanced fibrocavitary pulmonary sarcoidosis and chronic pulmonary aspergillosis.BMJ Case Rep. 2022 Aug 22;15(8):e250751. doi: 10.1136/bcr-2022-250751. BMJ Case Rep. 2022. PMID: 35995460 Free PMC article.
-
Non-Infectious Granulomatous Lung Disease: Imaging Findings with Pathologic Correlation.Korean J Radiol. 2021 Aug;22(8):1416-1435. doi: 10.3348/kjr.2020.1082. Epub 2021 May 26. Korean J Radiol. 2021. PMID: 34132073 Free PMC article. Review.
References
-
- Pant K, Chawla R, Shah A, et al. . Fibrebronchoscopy in pulmonary sarcoidosis—an Indian experience. Indian J Chest Dis Allied Sci 1990;32:199–203 - PubMed
-
- Shah A. [Editorial] Is sarcoidosis still uncommon in India? Indian J Chest Dis Allied Sci 2003;45:93–5 - PubMed
-
- Mayock RL, Bertrand P, Morrison CE, et al. . Manifestations of sarcoidosis. Analysis of 145 patients, with a review of nine series selected from the literature. Am J Med 1963;35:67–89 - PubMed
-
- Hours S, Nunes H, Kambouchner M, et al. . Pulmonary cavitary sarcoidosis: clinico-radiologic characteristics and natural history of a rare form of sarcoidosis. Medicine (Baltimore) 2008;87:142–51 - PubMed
-
- Gupta SK, Gupta S. Sarcoidosis in India: a review of 125 biopsy-proven cases from eastern India. Sarcoidosis 1990;7:43–9 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources