

Choosing algorithms for TB screening: a modelling study to compare yield, predictive value and diagnostic burden
- PMID: 25326816
- PMCID: PMC4287425
- DOI: 10.1186/1471-2334-14-532
Choosing algorithms for TB screening: a modelling study to compare yield, predictive value and diagnostic burden
Abstract
Background: To inform the choice of an appropriate screening and diagnostic algorithm for tuberculosis (TB) screening initiatives in different epidemiological settings, we compare algorithms composed of currently available methods.
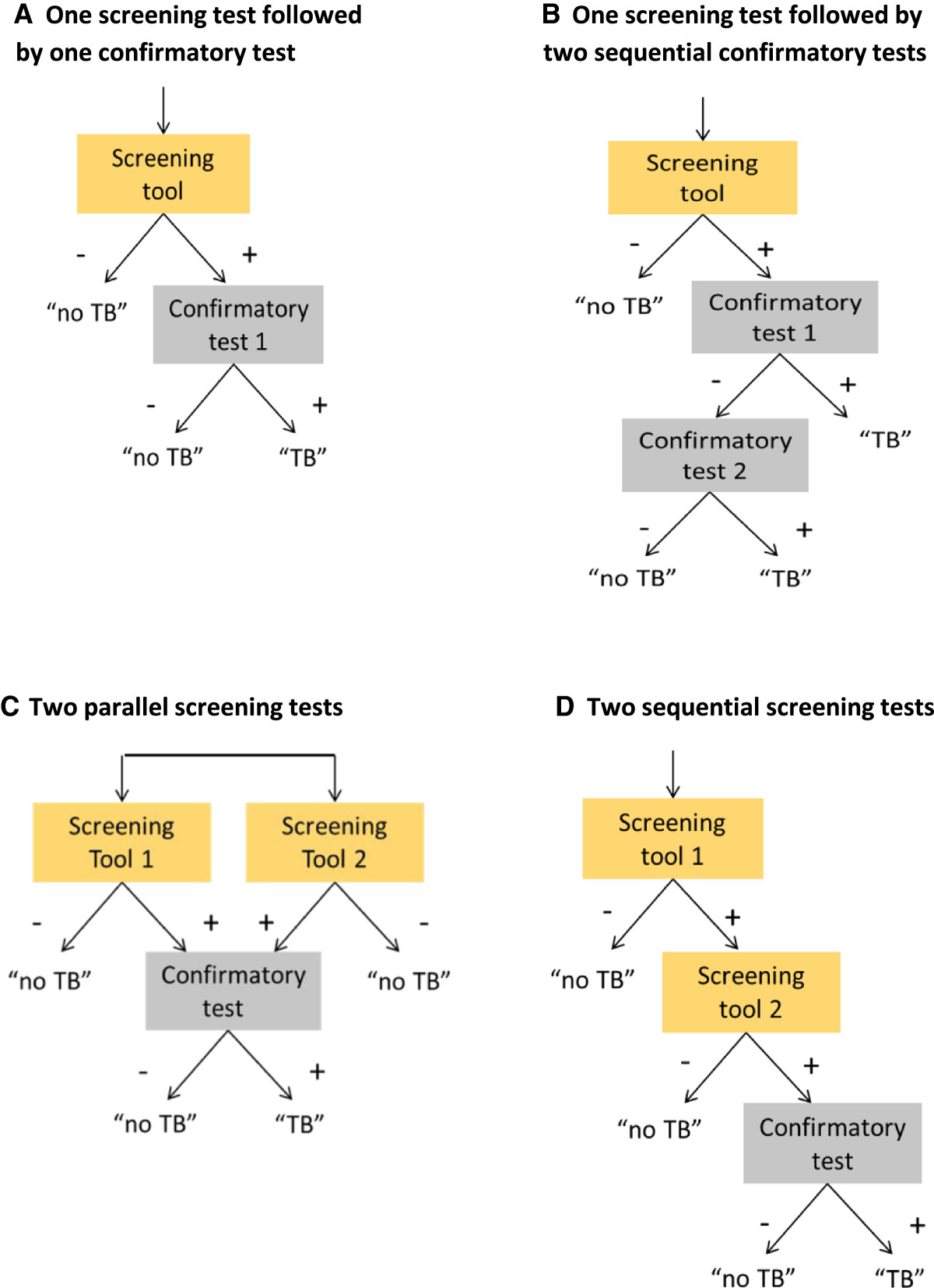
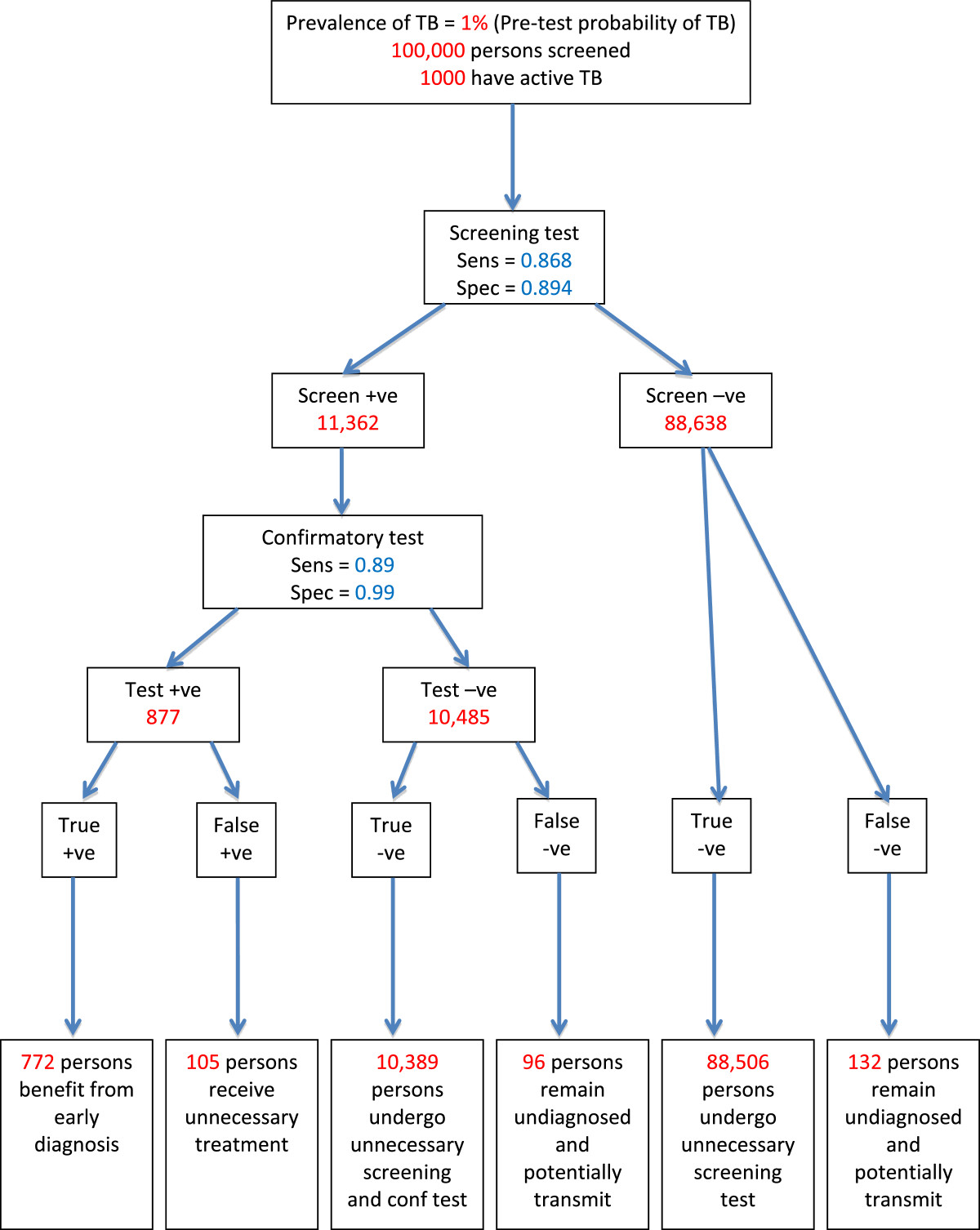
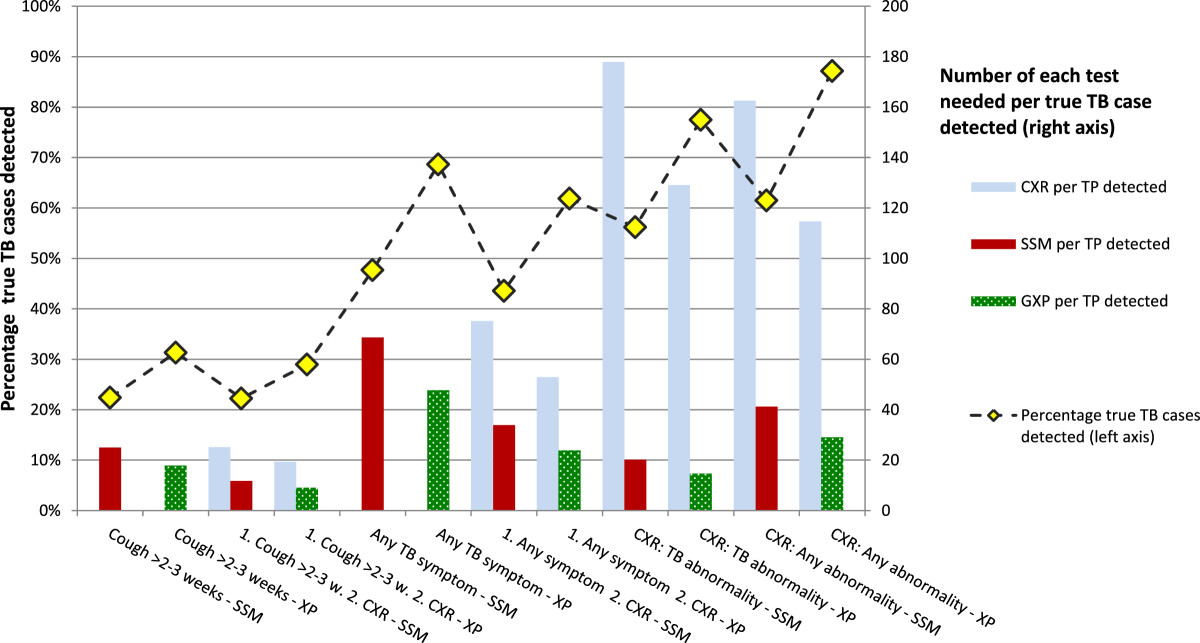
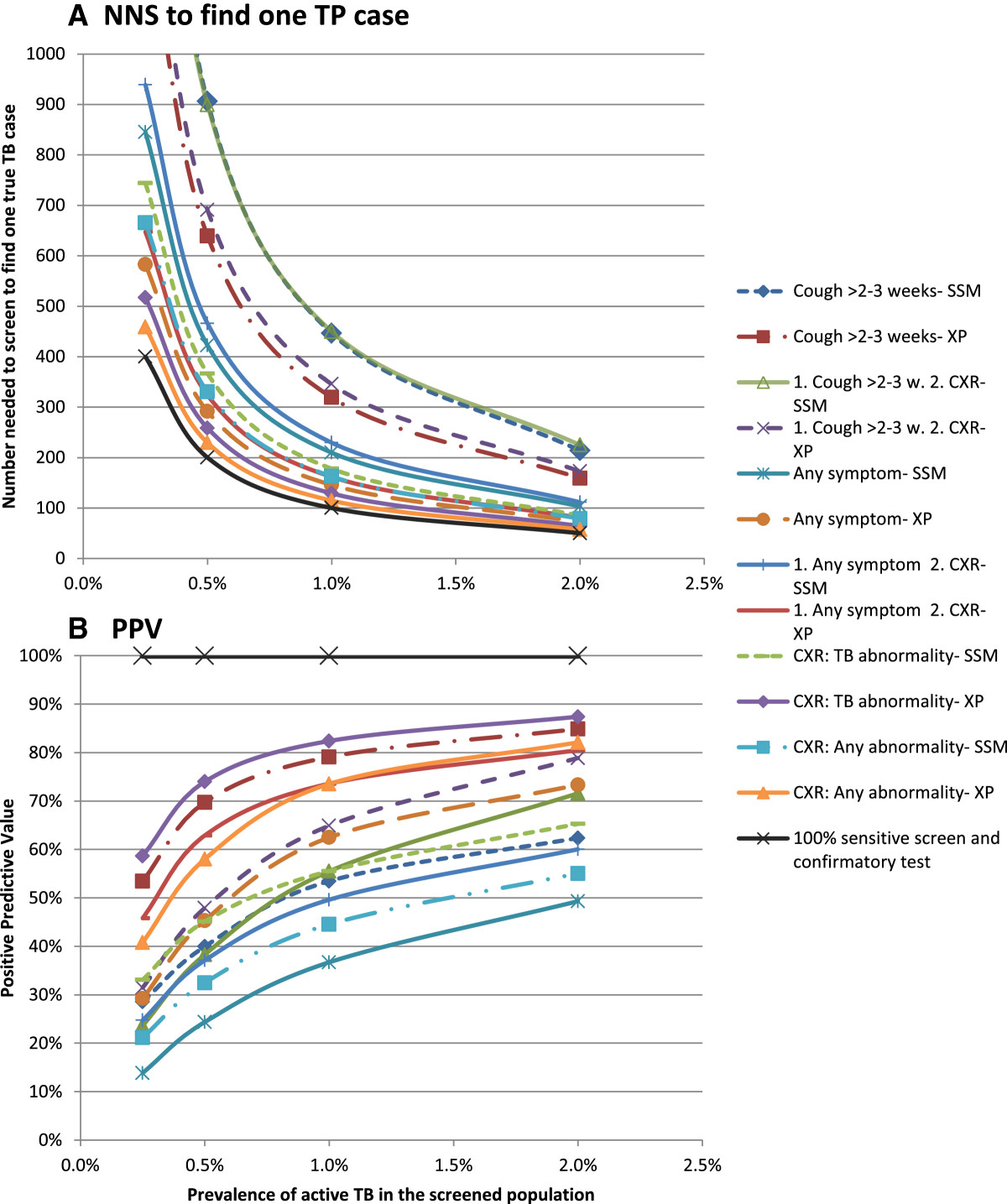
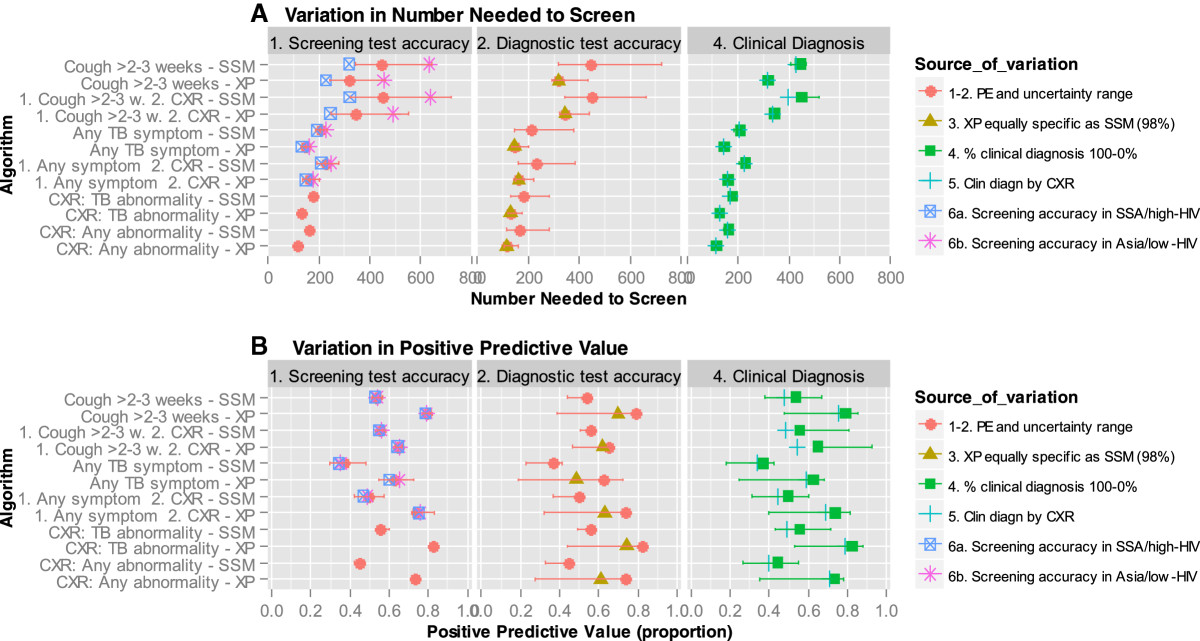
Methods: Of twelve algorithms composed of screening for symptoms (prolonged cough or any TB symptom) and/or chest radiography abnormalities, and either sputum-smear microscopy (SSM) or Xpert MTB/RIF (XP) as confirmatory test we model algorithm outcomes and summarize the yield, number needed to screen (NNS) and positive predictive value (PPV) for different levels of TB prevalence.
Results: Screening for prolonged cough has low yield, 22% if confirmatory testing is by SSM and 32% if XP, and a high NNS, exceeding 1000 if TB prevalence is ≤0.5%. Due to low specificity the PPV of screening for any TB symptom followed by SSM is less than 50%, even if TB prevalence is 2%. CXR screening for TB abnormalities followed by XP has the highest case detection (87%) and lowest NNS, but is resource intensive. CXR as a second screen for symptom screen positives improves efficiency.
Conclusions: The ideal algorithm does not exist. The choice will be setting specific, for which this study provides guidance. Generally an algorithm composed of CXR screening followed by confirmatory testing with XP can achieve the lowest NNS and highest PPV, and is the least amenable to setting-specific variation. However resource requirements for tests and equipment may be prohibitive in some settings and a reason to opt for symptom screening and SSM. To better inform disease control programs we need empirical data to confirm the modeled yield, cost-effectiveness studies, transmission models and a better screening test.
Figures
References
-
- World Health Organization . Global Tuberculosis Report 2013. Geneva: World Health Organization; 2013.
-
- World Health Organization . Systematic Screening for Active Tuberculosis. Principles and Recommendations. Geneva: World Health Organization; 2013. - PubMed
-
- van’t Hoog AH, Langendam MW, Mitchell E, Cobelens FG, Sinclair D, Leeflang MMG, Lonnroth K. A Systematic Review of the Sensitivity and Specificity of Symptom- and Chest-Radiography Screening for Active Pulmonary Tuberculosis in HIV-Negative Persons and Persons with Unknown HIV Status. 2013. Report to WHO.
Pre-publication history
-
- The pre-publication history for this paper can be accessed here:http://www.biomedcentral.com/1471-2334/14/532/prepub
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
