

Clinical problems of colorectal cancer and endometrial cancer cases with unknown cause of tumor mismatch repair deficiency (suspected Lynch syndrome)
- PMID: 25328415
- PMCID: PMC4199650
- DOI: 10.2147/TACG.S48625
Clinical problems of colorectal cancer and endometrial cancer cases with unknown cause of tumor mismatch repair deficiency (suspected Lynch syndrome)
Abstract
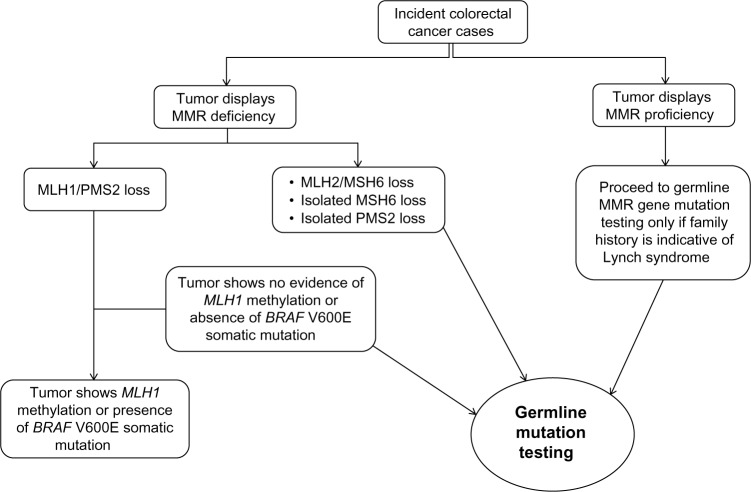
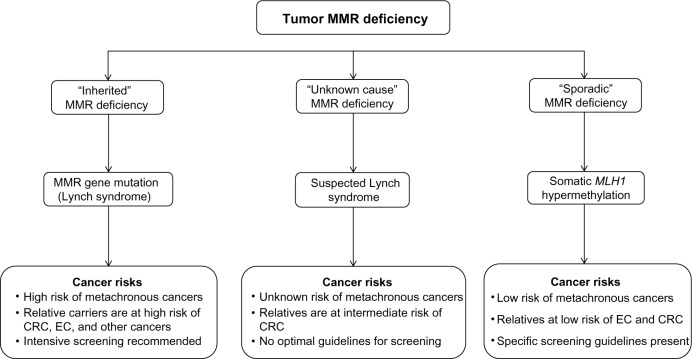
Carriers of a germline mutation in one of the DNA mismatch repair (MMR) genes have a high risk of developing numerous different cancers, predominantly colorectal cancer and endometrial cancer (known as Lynch syndrome). MMR gene mutation carriers develop tumors with MMR deficiency identified by tumor microsatellite instability or immunohistochemical loss of MMR protein expression. Tumor MMR deficiency is used to identify individuals most likely to carry an MMR gene mutation. However, MMR deficiency can also result from somatic inactivation, most commonly methylation of the MLH1 gene promoter. As tumor MMR testing of all incident colorectal and endometrial cancers (universal screening) is becoming increasingly adopted, a growing clinical problem is emerging for individuals who have tumors that show MMR deficiency who are subsequently found not to carry an MMR gene mutation after genetic testing using the current diagnostic approaches (Sanger sequencing and multiplex ligation-dependent probe amplification) and who also show no evidence of MLH1 methylation. The inability to determine the underlying cause of tumor MMR deficiency in these "Lynch-like" or "suspected Lynch syndrome" cases has significant implications on the clinical management of these individuals and their relatives. When the data from published studies are combined, 59% (95% confidence interval [CI]: 55% to 64%) of colorectal cancers and 52% (95% CI: 41% to 62%) of endometrial cancers with MMR deficiency were identified as suspected Lynch syndrome. Recent studies estimated that colorectal cancer risk for relatives of suspected Lynch syndrome cases is lower than for relatives of those with MMR gene mutations, but higher than for relatives of those with tumor MMR deficiency resulting from methylation of the MLH1 gene promoter. The cause of tumor MMR deficiency in suspected Lynch syndrome cases is likely due to either unidentified germline MMR gene mutations, somatic cell mosaicism, or biallelic somatic inactivation. Determining the underlying cause of tumor MMR deficiency in suspected Lynch syndrome cases is likely to reshape the current triaging schemes used to identify germline MMR gene mutations in cancer-affected individuals and their relatives.
Keywords: Lynch syndrome; cancer risk; germline mutation; screening; somatic mutation.
Figures
References
-
- Rustgi AK. The genetics of hereditary colon cancer. Genes Dev. 2007;21(20):2525–2538. - PubMed
-
- Buchanan DD, Tan YY, Walsh MD, et al. Tumor mismatch repair immunohistochemistry and DNA MLH1 methylation testing of patients with endometrial cancer diagnosed at age younger than 60 years optimizes triage for population-level germline mismatch repair gene mutation testing. J Clin Oncol. 2014;32(2):90–100. - PMC - PubMed
-
- Ligtenberg MJ, Kuiper RP, Chan TL, et al. Heritable somatic methylation and inactivation of MSH2 in families with Lynch syndrome due to deletion of the 3′ exons of TACSTD1. Nat Genet. 2009;41(1):112–117. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
