

Impingement and dislocation in total hip arthroplasty: mechanisms and consequences
- PMID: 25328453
- PMCID: PMC4127709
Impingement and dislocation in total hip arthroplasty: mechanisms and consequences
Abstract
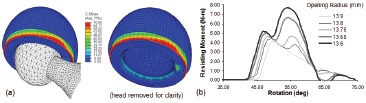
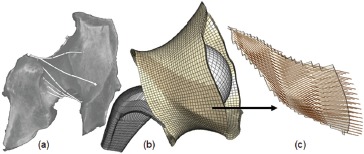
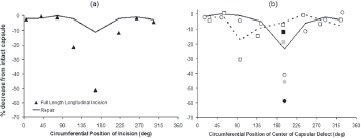
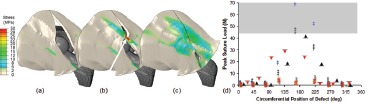
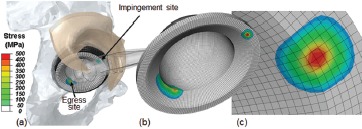
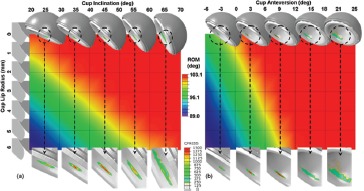
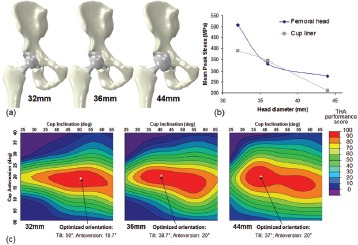
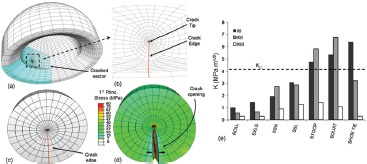
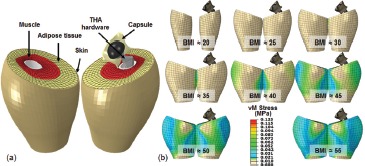
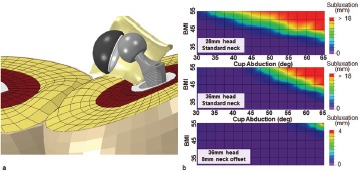
In contemporary total hip arthroplasty, instability has been a complication in approximately 2% to 5% of primary surgeries and 5% to 10% of revisions. Due to the reduction in the incidence of wear-induced osteolysis that has been achieved over the last decade, instability now stands as the single most common reason for revision surgery. Moreover, even without frank dislocation, impingement and subluxation are implicated in a set of new concerns arising with advanced bearings, associated with the relatively unforgiving nature of many of those designs. Against that backdrop, the biomechanical factors responsible for impingement, subluxation, and dislocation remain under-investigated relative to their burden of morbidity. This manuscript outlines a 15-year program of laboratory and clinical research undertaken to improve the scientific basis for understanding total hip impingement and dislocation. The broad theme has been to systematically evaluate the role of surgical factors, implant design factors, and patient factors in predisposing total hip constructs to impinge, sublux, and/or dislocate. Because this class of adverse biomechanical events had not lent itself well to study with existing approaches, it was necessary to develop (and validate) a series of new research methodologies, relying heavily on advanced finite element formulations. Specific areas of focus have included identifying the biomechanical challenges posed by dislocation-prone patient activities, quantifying design parameter effects and component surgical positioning effects for conventional metal-on-polyethylene implant constructs, and the impingement/dislocation behavior of non-conventional constructs, quantifying the stabilizing role of the hip capsule (and of surgical repairs of capsule defects), and systematically studying impingement and edge loading of hard-on-hard bearings, fracture of ceramic liners, confounding effects of patient obesity, and subluxation-mediated worsening of third body particle challenge.
Figures



References
-
- Bozic KJ, Kurtz SM, Lau E, Ong K, Vail TP, Berry DJ. The epidemiology of revision total hip arthroplasty in the United States. J.Bone Joint Surg. Am. 2009;91:128–133. - PubMed
-
- Alberton GM, High WA, Morrey BF. Dislocation after revision total hip arthroplasty: An analysis of risk factors and treatment options. J Bone Joint Surg Am. 2002;84:1788–1792. - PubMed
-
- Sanchez-Sotelo J, Berry DJ. Epidemiology of instability after total hip replacement. Orthop.Clin. North Am. 2001;32:543–52. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical