

A review of the role of simulation in developing and assessing orthopaedic surgical skills
- PMID: 25328480
- PMCID: PMC4127711
A review of the role of simulation in developing and assessing orthopaedic surgical skills
Abstract
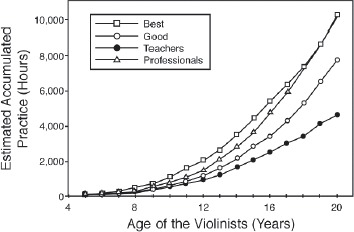
Orthopaedic surgical skill is traditionally acquired during training in an apprenticeship model that has been largely unchanged for nearly 100 years. However, increased pressure for operating room efficiency, a focus on patient safety, work hour restrictions, and a movement towards competency-based education are changing the traditional paradigm. Surgical simulation has the potential to help address these changes. This manuscript reviews the scientific background on skill acquisition and surgical simulation as it applies to orthopaedic surgery. It argues that simulation in orthopaedics lags behind other disciplines and focuses too little on simulator validation. The case is made that orthopaedic training is more efficient with simulators that facilitate deliberate practice throughout resident training and more research should be focused on simulator validation and the refinement of skill definition.
Figures


References
-
- Flood AB, Scott WR, Ewy W. Does practice make perfect? Part I: The relation between hospital volume and outcomes for selected diagnostic categories. Med Care. 1984;22(2):98–114. - PubMed
-
- Flood AB, Scott WR, Ewy W. Does practice make perfect? Part II: The relation between volume and and outcomes and other hospital characteristics. Med Care. 1984;22(2):115–125. - PubMed
-
- Luft HS. The relation between surgical volume and mortality: An exploration of causal factors and alternative models. Med Care. 1980;18(9):940–959. - PubMed
-
- Luft HS, Bunker JP, Enthoven AC. Should operations be regionalized? The empirical relation between surgical volume and mortality. New Eng J Med. 1979;301(25):1364–1369. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources